{"title":"Brentuximab vedotin treatment for mycosis fungoides with CD30+ large-cell transformation in the early stage","authors":"Shujiro Hayashi MD, PhD, Shown Tokoro MD, Ken Igawa MD, PhD","doi":"10.1002/cia2.12330","DOIUrl":null,"url":null,"abstract":"<p>Mycosis fungoides (MF), the most common type of cutaneous T-cell lymphoma, is characterized by the proliferation of small- to medium-sized atypical, usually CD4+ T cells in the skin.<span><sup>1</sup></span> Mycosis fungoides with large-cell transformation (LCT) is an aggressive subtype defined by the presence of large cells comprising >25% of the lesion infiltrate or the presence of microscopic nodules of large cells. Large-cell transformation occurs in 20%–55% of advanced MF cases and is often a histological marker of poor prognosis and is associated with a mean 5-year survival rate of <20%.<span><sup>1</sup></span> Herein, we present a patient with MF-LCT in its early stage that was successfully treated with brentuximab vedotin (BV), an anti-CD30 antibody.</p><p>A woman in her early 30s had erythema with pruritus and pigmentation on her trunk and thighs for 3 years (Figure 1A). Following subsequent histopathological diagnosis as MF (negative CD30+ lymphocytes at this time), she was successfully treated with topical steroids and ultraviolet therapy and showed no progression for approximately 10 years. In her early 40s, the rash slowly expanded and was treated with bexarotene (450–150 mg/day). One year later, the eruption intensified, with erythema observed on 40% of the body and multiple skin tumors of ≥1 cm (Figure 1B,C). Histopathology and immunohistochemistry of the tumors confirmed infiltration with CD3+, CD4+, CD5+, CD8+ (CD4/CD8: 10/1), CD30+, and CD20− lymphocytes, and CD30+ lymphocytes with large nuclei comprised 30% of the infiltrate (Figure 1D,E). The patient's complete blood count was normal, and the peripheral blood smear was negative for Sézary cells. Bone marrow examination showed no infiltration of atypical lymphocytes. No lymph node metastasis was found on positron emission tomography–computed tomography. Mycosis fungoides stage IIB (T3M0N0) with CD30+ LCT was diagnosed, and BV treatment was initiated instead of bexarotene. After three doses, the eruption area decreased, and the nodules became flattened (Figure 1E,F). After a total of 16 BV treatments, the only side effect observed was mild sensory polyneuropathy.</p><p>Brentuximab vedotin is an antibody–drug conjugate (ADC) in which monomethyl auristatin E (MMAE), which has cytotoxic activity, and an anti-CD30 IgG1-type chimeric antibody are linked via a protease-cleavable linker. The ADC inhibits tumor growth by first binding to CD30+ cells. Then, after being taken up into the cells as an ADC–CD30 complex, it releases MMAE through a proteolytic reaction. The free MMAE further inhibits microtubule formation and induces cell cycle arrest and apoptosis.<span><sup>2</sup></span> In a clinical trial of 30 patients (MF and Sézary syndrome), the response rate for BV was 70%, wherein 54% of the respondents were free of disease progression for 1 year<span><sup>3</sup></span>; however, the information on MF-LCT is still limited.</p><p>Bhari N et al. reported that the survival prognosis of 11 cases of MF in which transformation was diagnosed in the early stage was reported as good.<span><sup>4</sup></span> Stage IIB has a significantly worse 5-year survival rate compared with stage IB/IIA, which often plagues clinicians regarding appropriate treatment selection.<span><sup>5</sup></span> In our case, the discovery of LCT warranted treatment with BV. Therefore, proactive rebiopsy is important for CD30+ LCT to not be overlooked.</p><p>The authors declare no conflict of interest.</p><p>Approval of the research protocol: No human participant was involved in this study.</p><p>Informed Consent: Informed consent was obtained from the patient.</p><p>Registry and registration No. of this study/trials: N/A.</p><p>Animal studies: N/A.</p>","PeriodicalId":15543,"journal":{"name":"Journal of Cutaneous Immunology and Allergy","volume":"6 6","pages":"260-261"},"PeriodicalIF":0.9000,"publicationDate":"2023-09-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cia2.12330","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cutaneous Immunology and Allergy","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cia2.12330","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"ALLERGY","Score":null,"Total":0}
引用次数: 0
Abstract
Mycosis fungoides (MF), the most common type of cutaneous T-cell lymphoma, is characterized by the proliferation of small- to medium-sized atypical, usually CD4+ T cells in the skin.1 Mycosis fungoides with large-cell transformation (LCT) is an aggressive subtype defined by the presence of large cells comprising >25% of the lesion infiltrate or the presence of microscopic nodules of large cells. Large-cell transformation occurs in 20%–55% of advanced MF cases and is often a histological marker of poor prognosis and is associated with a mean 5-year survival rate of <20%.1 Herein, we present a patient with MF-LCT in its early stage that was successfully treated with brentuximab vedotin (BV), an anti-CD30 antibody.
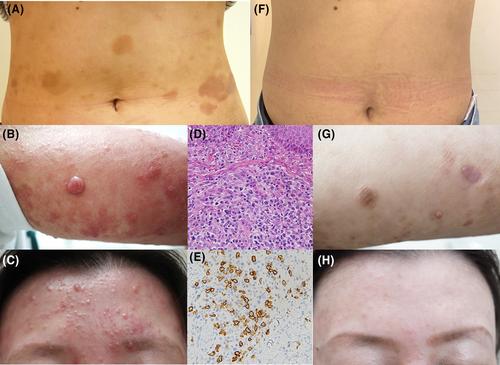
A woman in her early 30s had erythema with pruritus and pigmentation on her trunk and thighs for 3 years (Figure 1A). Following subsequent histopathological diagnosis as MF (negative CD30+ lymphocytes at this time), she was successfully treated with topical steroids and ultraviolet therapy and showed no progression for approximately 10 years. In her early 40s, the rash slowly expanded and was treated with bexarotene (450–150 mg/day). One year later, the eruption intensified, with erythema observed on 40% of the body and multiple skin tumors of ≥1 cm (Figure 1B,C). Histopathology and immunohistochemistry of the tumors confirmed infiltration with CD3+, CD4+, CD5+, CD8+ (CD4/CD8: 10/1), CD30+, and CD20− lymphocytes, and CD30+ lymphocytes with large nuclei comprised 30% of the infiltrate (Figure 1D,E). The patient's complete blood count was normal, and the peripheral blood smear was negative for Sézary cells. Bone marrow examination showed no infiltration of atypical lymphocytes. No lymph node metastasis was found on positron emission tomography–computed tomography. Mycosis fungoides stage IIB (T3M0N0) with CD30+ LCT was diagnosed, and BV treatment was initiated instead of bexarotene. After three doses, the eruption area decreased, and the nodules became flattened (Figure 1E,F). After a total of 16 BV treatments, the only side effect observed was mild sensory polyneuropathy.
Brentuximab vedotin is an antibody–drug conjugate (ADC) in which monomethyl auristatin E (MMAE), which has cytotoxic activity, and an anti-CD30 IgG1-type chimeric antibody are linked via a protease-cleavable linker. The ADC inhibits tumor growth by first binding to CD30+ cells. Then, after being taken up into the cells as an ADC–CD30 complex, it releases MMAE through a proteolytic reaction. The free MMAE further inhibits microtubule formation and induces cell cycle arrest and apoptosis.2 In a clinical trial of 30 patients (MF and Sézary syndrome), the response rate for BV was 70%, wherein 54% of the respondents were free of disease progression for 1 year3; however, the information on MF-LCT is still limited.
Bhari N et al. reported that the survival prognosis of 11 cases of MF in which transformation was diagnosed in the early stage was reported as good.4 Stage IIB has a significantly worse 5-year survival rate compared with stage IB/IIA, which often plagues clinicians regarding appropriate treatment selection.5 In our case, the discovery of LCT warranted treatment with BV. Therefore, proactive rebiopsy is important for CD30+ LCT to not be overlooked.
The authors declare no conflict of interest.
Approval of the research protocol: No human participant was involved in this study.
Informed Consent: Informed consent was obtained from the patient.
Registry and registration No. of this study/trials: N/A.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
