LDL-C rebound after long-term evolocumab treatment and intravascular imaging evidence in a familial hypercholesterolemia patient with early-onset myocardial infarction
{"title":"LDL-C rebound after long-term evolocumab treatment and intravascular imaging evidence in a familial hypercholesterolemia patient with early-onset myocardial infarction","authors":"Zhifan Li, Shuang Zhang, Zheng Yin, Wenjia Zhang, Yonggang Sui, Jianjun Li, Kefei Dou, Jie Qian, Naqiong Wu","doi":"10.1002/cdt3.97","DOIUrl":null,"url":null,"abstract":"<p>Patients with familial hypercholesterolemia (FH) have elevated low-density lipoprotein cholesterol (LDL-C) levels and are at high risk of premature cardiovascular disease.<span><sup>1</sup></span> Heterozygous FH (HeFH) is one of the commonest genetic disorders, and is more frequent among those with ischemic heart disease (IHD), atherosclerotic cardiovascular disease (ASCVD) and premature IHD.<span><sup>2</sup></span> FH screening, followed by effective lipid-lowering therapy (LLT) including proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor can slow or even reverse plaque progression and reduce risk.<span><sup>3</sup></span></p><p>Optical coherence tomography (OCT) is a promising intravascular approach in visualizing coronary plaque morphology, assessing disease progression, and monitoring response to treatments with high axial resolution (10–15 µm).<span><sup>4</sup></span> Several related clinical trials have demonstrated that statins alone or in combination with PCSK9 inhibitors produce regression of atherosclerosis.<span><sup>5-7</sup></span></p><p>Here, we presented a patient with premature IHD, who was a probable HeFH and received evolocumab (Repatha®) after percutaneous coronary intervention (PCI). We followed his clinical and laboratory results for over 3.5 years, and used OCT to monitor vascular response to PCSK9 inhibitor treatment.</p><p>A 34-year-old man with hyperlipidemia and hypertension self-presented to the emergency department due to exertional chest pain for 3 days on November 23, 2019. His height, body weight, and body mass index were 170 cm, 95 kg, and 32.9 kg/m<sup>2</sup>, respectively. Cardiac troponin I (cTnI) was mildly elevated at 0.297 ng/mL, and electrocardiogram demonstrated ST-T changes in I, aVL, II, III, aVF, V5–V9 leads, suggesting acute inferior, lateral, and posterior myocardial infarction. After medical stabilization, he underwent coronary angiography (CAG), revealing triple vessel disease (Figure 1) and received percutaneous transluminal coronary angioplasty to the left circumflex artery (LCX) with a stent on November 24, and another drug balloon dilation at posterior descending artery (PDA) on December 3. Standard postoperative treatment was given and the patient had no episodes of chest tightness accompanied by a regression of cTnI.</p><p>Laboratory examinations showed that his LDL-C and triglyceride (TG) levels were upper normal (Figure 2). Considering his LDL-C level remained at 3.45 mmol/L after combined oral LLT (statin + ezetimibe), we estimated his baseline LDL-C to be over 6.50 mmol/L. Besides, his father has a history of hyperlipidemia and PCI. According to the criteria of the Dutch Lipid Clinic Network (DLCN),<span><sup>8</sup></span> the patient could be diagnosed as probable FH (his DLCN score = 8).</p><p>Based on early onset acute coronary syndromes (ACS) combined with multiple high-risk conditions, the patient could be defined as very high-risk ASCVD patient according to American Heart Association/American College of Cardiology guideline,<span><sup>9</sup></span> and was managed with evolocumab, a PCSK9 monoclonal antibody, 140 mg subcutaneously every 2 weeks on the basis of statin and ezetimibe therapy (rosuvastatin 10 mg qn + ezetimibe 10 mg qd). The above LLT lowered his LDL-C levels by 42%–50% in the first year, which maintained at 1.74–1.99 mmol/L (Figure 2). Similar to the changes in LDL-C, his total cholesterol, TG, and apolipoprotein B also decreased by about 50%. High-density lipoprotein cholesterol increased slightly (from 0.75 mmol/L to about 1 mmol/L), while lipoprotein(a) decreased in the first month, then increased to more than double in the next 3 months, and then decreased to slightly above baseline levels (Figure 2).</p><p>On November 10, 2020, the patient was admitted for a 1-year re-examination. He reported no recurrent symptoms and normal in physical and laboratory examinations. CAG showed that the original LCX artery stent was patent, and there was no restenosis at the drug balloon treatment site of PDA artery. The left anterior descending artery (LAD) stenosis did not progress, and a drug balloon dilation was performed in the middle segment of the LAD. Meanwhile, OCT was performed to view proximal segment of LAD, suggesting dissection, but not involving the middle membrane (Figure 3A). Due to fluctuations in LDL-C levels with evolocumab 140 mg biweekly and LDL-C levels not meeting the guideline recommendations for very high-risk patients, the patient's physician adjusted the dose of evolocumab to 140 mg subcutaneously every 10 days. For the next 3 months, his LDL-C levels decreased by 57%–60% from baseline, maintained at 1.39–1.54 mmol/L (Figure 2).</p><p>When the patient was hospitalized for a 2-year thorough examination on November 8, 2021, CAG showed no progression in stenosis and OCT showed a trend of thickening of the fibrous cap and a shift in plaque properties from lipid to fibrous (Figure 3B). However, his LDL level rebounded to 2.30 mmol/L. In March 2022, the patient consulted for lipid-lowering and weight loss, which increased from 88 to 98 kg in the past year. He reported no changes in his lifestyle or medication use other than an increase in dietary intake. We adjusted evolocumab to 420 mg once a month (three injections at a time) according to guidelines for FH patients, and advised the patient to lose weight and inject liraglutide (a glucagon-like peptide-1 receptor agonist) regularly. After 2 months, the patient lost 5 kg of weight, and LDL-C decreased from 2.79 to 2.05 mmol/L, which had further reduced to 1.82 mmol/L in August 2022 (Figure 2). In December, the patient reported that his appetite increased greatly and his weight gained after recovery from SARS-CoV-2 Omicron infection. His LDL-C level raised up again and maintained at about 2.35 mmol/L in recent 8 months (Figure 2).</p><p>Hypercholesterolemia is an independent risk factor for cardiovascular diseases. Intensive LLT can significantly reduce the risk of ASCVD morbidity and mortality, especially in patients with high baseline LDL-C levels.<span><sup>10</sup></span> FH patients are more likely to develop atherosclerosis and early-onset cardiovascular events due to inadequate LLT.<span><sup>11</sup></span> Numerous studies have shown dose-dependent associations between LDL-C levels and the risk of cardiovascular events and recurrence, and that lowering LDL-C reduces the risk of major cardiovascular events.<span><sup>12</sup></span> Currently, several guidelines for lipid management recommend population risk stratification and appropriate lipid-lowering targets.<span><sup>9, 13-15</sup></span> For secondary prevention, if LDL-C remained ≥70 mg/dL (1.8 mmol/L) after treatment with the maximum tolerated dose of statin plus ezetimibe, PCSK9 inhibitors may be considered.<span><sup>9</sup></span></p><p>PCSK9 is mainly synthetized in the liver and plays an important role in cholesterol metabolism by inhibiting low-density lipoprotein receptors (LDLR) recycling.<span><sup>16</sup></span> It is also intertwined with endothelial cell apoptosis, autophagy, platelet activation and aggregation, reduction of vascular stability, and local inflammation of atherosclerosis.<span><sup>17, 18</sup></span> PCSK9 inhibitors can increase the expression of LDLR on the surface of hepatic cells with the resultant decrease in plasma LDL-C, thus reducing the incidence of ASCVD events.<span><sup>19</sup></span> Considering that this ACS patient had received statin and ezetimibe, LDL-C targets were still not reached, so we added PCSK9 inhibitor early in his hospital stay to improve the lipid-lowering efficacy. It is worth mentioning that evolocumab (Repatha®) is the first PCSK9 inhibitor approved for marketing in China, and was approved for a wider range of indications including pre-existing ASCVD and HeFH on November 22, 2019. Therefore, this patient is one of the first local patients to receive evolocumab and has been using it continuously for more than 3.5 years.</p><p>OCT is a high-resolution intravascular imaging technique that provides accurate values of diseased vessels, identifies plaque pathology, and helps to accurately determine lesions, assess stent effectiveness, and detect plaque healing for clinical benefit.<span><sup>5</sup></span> The recently published HUYGENS study demonstrated that early combination of intensive LLT with evolocumab for 1 year after ACS significantly increased the minimum fibrous cap thickness and reduced the maximum lipid arc and macrophage index in vulnerable plaques in coronary arteries.<span><sup>7</sup></span> This suggests that we may consider early initiation of the combination therapy with evolocumab in very high-risk patients. Excitingly, OCT confirmed that our patient's plaques turned stable.</p><p>Notably, the patient showed LDL-C rebound after receiving evolocumab. The first thing to consider was whether he developed resistance to PCSK9 monoclonal antibody. In the Studies of PCSK9 Inhibition and the Reduction of Vascular Events, LDL-C reduction was attenuated over time due to the presence of antibodies for another PCSK9 inhibitor “bococizumab.”<span><sup>20</sup></span> Neutralizing antibody assay was not performed in this case due to limited conditions, and current studies did not find any resistance to evolocumab.<span><sup>21</sup></span> Besides, the recent FOURIER-Open-label-extension study showed a strong and sustained reduction in LDL-C for up to 8.4 years after using evolocumab, with no neutralizing antibodies detected.<span><sup>22</sup></span></p><p>Additionally, the patient gained weight after 1.5 years of medication. After weight loss, LDL-C decreased again by maintaining the same dose of evolocumab (420 mg monthly), suggesting that evolocumab still has a good lipid-lowering effect. However, the patient's weight regained after Omicron infection, and his LDL-C level also rebounded despite the maximum dose of evolocumab (420 mg ih qm). The China Health and Nutrition Survey showed that adults with higher dietary cholesterol intake had higher odds of hypercholesterolemia, and energy intake from animal protein was positively associated with LDL-C.<span><sup>23, 24</sup></span></p><p>Thus, obesity and unhealthy eating habits may be important causes of lipid fluctuations. We recommended the patient to a lifestyle specialty clinic, hoping that a professional lifestyle intervention with dietary control and significant weight loss will enable the patient to achieve optimal LDL-C reduction with evolocumab. This also suggests us that patient health education and lifestyle improvement are still important for lipid management at a time when more potent lipid-lowering medications are available.</p><p><i>Conception/design, manuscript review</i>: Naqiong Wu. <i>Provision of study materials, supervision</i>: Naqiong Wu, Wenjia Zhang, Yonggang Sui, Jianjun Li, Kefei Dou, Jie Qian. Collection and/or assembly of data, manuscript preparation: Shuang Zhang, Zheng Yin, and Zhifan Li. <i>Data analysis, visualization, interpretation, and manuscript writing</i>: Zhifan Li. All authors have read and agreed to the published version of the manuscript.</p><p>The authors declare no conflict of interest.</p><p>The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Fuwai Hospital. The authors certify that they have obtained patient consent forms.</p>","PeriodicalId":32096,"journal":{"name":"Chronic Diseases and Translational Medicine","volume":"10 1","pages":"69-74"},"PeriodicalIF":0.0000,"publicationDate":"2023-10-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cdt3.97","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chronic Diseases and Translational Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cdt3.97","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Patients with familial hypercholesterolemia (FH) have elevated low-density lipoprotein cholesterol (LDL-C) levels and are at high risk of premature cardiovascular disease.1 Heterozygous FH (HeFH) is one of the commonest genetic disorders, and is more frequent among those with ischemic heart disease (IHD), atherosclerotic cardiovascular disease (ASCVD) and premature IHD.2 FH screening, followed by effective lipid-lowering therapy (LLT) including proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor can slow or even reverse plaque progression and reduce risk.3
Optical coherence tomography (OCT) is a promising intravascular approach in visualizing coronary plaque morphology, assessing disease progression, and monitoring response to treatments with high axial resolution (10–15 µm).4 Several related clinical trials have demonstrated that statins alone or in combination with PCSK9 inhibitors produce regression of atherosclerosis.5-7
Here, we presented a patient with premature IHD, who was a probable HeFH and received evolocumab (Repatha®) after percutaneous coronary intervention (PCI). We followed his clinical and laboratory results for over 3.5 years, and used OCT to monitor vascular response to PCSK9 inhibitor treatment.
A 34-year-old man with hyperlipidemia and hypertension self-presented to the emergency department due to exertional chest pain for 3 days on November 23, 2019. His height, body weight, and body mass index were 170 cm, 95 kg, and 32.9 kg/m2, respectively. Cardiac troponin I (cTnI) was mildly elevated at 0.297 ng/mL, and electrocardiogram demonstrated ST-T changes in I, aVL, II, III, aVF, V5–V9 leads, suggesting acute inferior, lateral, and posterior myocardial infarction. After medical stabilization, he underwent coronary angiography (CAG), revealing triple vessel disease (Figure 1) and received percutaneous transluminal coronary angioplasty to the left circumflex artery (LCX) with a stent on November 24, and another drug balloon dilation at posterior descending artery (PDA) on December 3. Standard postoperative treatment was given and the patient had no episodes of chest tightness accompanied by a regression of cTnI.
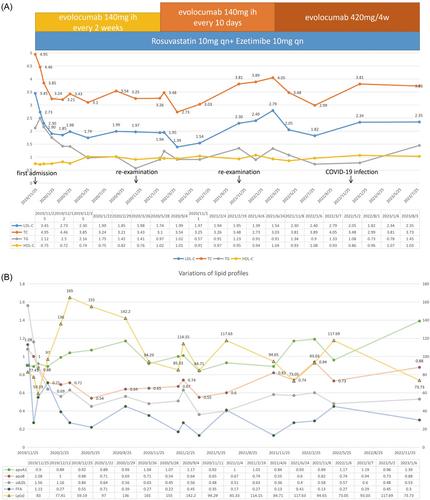
Laboratory examinations showed that his LDL-C and triglyceride (TG) levels were upper normal (Figure 2). Considering his LDL-C level remained at 3.45 mmol/L after combined oral LLT (statin + ezetimibe), we estimated his baseline LDL-C to be over 6.50 mmol/L. Besides, his father has a history of hyperlipidemia and PCI. According to the criteria of the Dutch Lipid Clinic Network (DLCN),8 the patient could be diagnosed as probable FH (his DLCN score = 8).
Based on early onset acute coronary syndromes (ACS) combined with multiple high-risk conditions, the patient could be defined as very high-risk ASCVD patient according to American Heart Association/American College of Cardiology guideline,9 and was managed with evolocumab, a PCSK9 monoclonal antibody, 140 mg subcutaneously every 2 weeks on the basis of statin and ezetimibe therapy (rosuvastatin 10 mg qn + ezetimibe 10 mg qd). The above LLT lowered his LDL-C levels by 42%–50% in the first year, which maintained at 1.74–1.99 mmol/L (Figure 2). Similar to the changes in LDL-C, his total cholesterol, TG, and apolipoprotein B also decreased by about 50%. High-density lipoprotein cholesterol increased slightly (from 0.75 mmol/L to about 1 mmol/L), while lipoprotein(a) decreased in the first month, then increased to more than double in the next 3 months, and then decreased to slightly above baseline levels (Figure 2).
On November 10, 2020, the patient was admitted for a 1-year re-examination. He reported no recurrent symptoms and normal in physical and laboratory examinations. CAG showed that the original LCX artery stent was patent, and there was no restenosis at the drug balloon treatment site of PDA artery. The left anterior descending artery (LAD) stenosis did not progress, and a drug balloon dilation was performed in the middle segment of the LAD. Meanwhile, OCT was performed to view proximal segment of LAD, suggesting dissection, but not involving the middle membrane (Figure 3A). Due to fluctuations in LDL-C levels with evolocumab 140 mg biweekly and LDL-C levels not meeting the guideline recommendations for very high-risk patients, the patient's physician adjusted the dose of evolocumab to 140 mg subcutaneously every 10 days. For the next 3 months, his LDL-C levels decreased by 57%–60% from baseline, maintained at 1.39–1.54 mmol/L (Figure 2).
When the patient was hospitalized for a 2-year thorough examination on November 8, 2021, CAG showed no progression in stenosis and OCT showed a trend of thickening of the fibrous cap and a shift in plaque properties from lipid to fibrous (Figure 3B). However, his LDL level rebounded to 2.30 mmol/L. In March 2022, the patient consulted for lipid-lowering and weight loss, which increased from 88 to 98 kg in the past year. He reported no changes in his lifestyle or medication use other than an increase in dietary intake. We adjusted evolocumab to 420 mg once a month (three injections at a time) according to guidelines for FH patients, and advised the patient to lose weight and inject liraglutide (a glucagon-like peptide-1 receptor agonist) regularly. After 2 months, the patient lost 5 kg of weight, and LDL-C decreased from 2.79 to 2.05 mmol/L, which had further reduced to 1.82 mmol/L in August 2022 (Figure 2). In December, the patient reported that his appetite increased greatly and his weight gained after recovery from SARS-CoV-2 Omicron infection. His LDL-C level raised up again and maintained at about 2.35 mmol/L in recent 8 months (Figure 2).
Hypercholesterolemia is an independent risk factor for cardiovascular diseases. Intensive LLT can significantly reduce the risk of ASCVD morbidity and mortality, especially in patients with high baseline LDL-C levels.10 FH patients are more likely to develop atherosclerosis and early-onset cardiovascular events due to inadequate LLT.11 Numerous studies have shown dose-dependent associations between LDL-C levels and the risk of cardiovascular events and recurrence, and that lowering LDL-C reduces the risk of major cardiovascular events.12 Currently, several guidelines for lipid management recommend population risk stratification and appropriate lipid-lowering targets.9, 13-15 For secondary prevention, if LDL-C remained ≥70 mg/dL (1.8 mmol/L) after treatment with the maximum tolerated dose of statin plus ezetimibe, PCSK9 inhibitors may be considered.9
PCSK9 is mainly synthetized in the liver and plays an important role in cholesterol metabolism by inhibiting low-density lipoprotein receptors (LDLR) recycling.16 It is also intertwined with endothelial cell apoptosis, autophagy, platelet activation and aggregation, reduction of vascular stability, and local inflammation of atherosclerosis.17, 18 PCSK9 inhibitors can increase the expression of LDLR on the surface of hepatic cells with the resultant decrease in plasma LDL-C, thus reducing the incidence of ASCVD events.19 Considering that this ACS patient had received statin and ezetimibe, LDL-C targets were still not reached, so we added PCSK9 inhibitor early in his hospital stay to improve the lipid-lowering efficacy. It is worth mentioning that evolocumab (Repatha®) is the first PCSK9 inhibitor approved for marketing in China, and was approved for a wider range of indications including pre-existing ASCVD and HeFH on November 22, 2019. Therefore, this patient is one of the first local patients to receive evolocumab and has been using it continuously for more than 3.5 years.
OCT is a high-resolution intravascular imaging technique that provides accurate values of diseased vessels, identifies plaque pathology, and helps to accurately determine lesions, assess stent effectiveness, and detect plaque healing for clinical benefit.5 The recently published HUYGENS study demonstrated that early combination of intensive LLT with evolocumab for 1 year after ACS significantly increased the minimum fibrous cap thickness and reduced the maximum lipid arc and macrophage index in vulnerable plaques in coronary arteries.7 This suggests that we may consider early initiation of the combination therapy with evolocumab in very high-risk patients. Excitingly, OCT confirmed that our patient's plaques turned stable.
Notably, the patient showed LDL-C rebound after receiving evolocumab. The first thing to consider was whether he developed resistance to PCSK9 monoclonal antibody. In the Studies of PCSK9 Inhibition and the Reduction of Vascular Events, LDL-C reduction was attenuated over time due to the presence of antibodies for another PCSK9 inhibitor “bococizumab.”20 Neutralizing antibody assay was not performed in this case due to limited conditions, and current studies did not find any resistance to evolocumab.21 Besides, the recent FOURIER-Open-label-extension study showed a strong and sustained reduction in LDL-C for up to 8.4 years after using evolocumab, with no neutralizing antibodies detected.22
Additionally, the patient gained weight after 1.5 years of medication. After weight loss, LDL-C decreased again by maintaining the same dose of evolocumab (420 mg monthly), suggesting that evolocumab still has a good lipid-lowering effect. However, the patient's weight regained after Omicron infection, and his LDL-C level also rebounded despite the maximum dose of evolocumab (420 mg ih qm). The China Health and Nutrition Survey showed that adults with higher dietary cholesterol intake had higher odds of hypercholesterolemia, and energy intake from animal protein was positively associated with LDL-C.23, 24
Thus, obesity and unhealthy eating habits may be important causes of lipid fluctuations. We recommended the patient to a lifestyle specialty clinic, hoping that a professional lifestyle intervention with dietary control and significant weight loss will enable the patient to achieve optimal LDL-C reduction with evolocumab. This also suggests us that patient health education and lifestyle improvement are still important for lipid management at a time when more potent lipid-lowering medications are available.
Conception/design, manuscript review: Naqiong Wu. Provision of study materials, supervision: Naqiong Wu, Wenjia Zhang, Yonggang Sui, Jianjun Li, Kefei Dou, Jie Qian. Collection and/or assembly of data, manuscript preparation: Shuang Zhang, Zheng Yin, and Zhifan Li. Data analysis, visualization, interpretation, and manuscript writing: Zhifan Li. All authors have read and agreed to the published version of the manuscript.
The authors declare no conflict of interest.
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Fuwai Hospital. The authors certify that they have obtained patient consent forms.
期刊介绍:
This journal aims to promote progress from basic research to clinical practice and to provide a forum for communication among basic, translational, and clinical research practitioners and physicians from all relevant disciplines. Chronic diseases such as cardiovascular diseases, cancer, diabetes, stroke, chronic respiratory diseases (such as asthma and COPD), chronic kidney diseases, and related translational research. Topics of interest for Chronic Diseases and Translational Medicine include Research and commentary on models of chronic diseases with significant implications for disease diagnosis and treatment Investigative studies of human biology with an emphasis on disease Perspectives and reviews on research topics that discuss the implications of findings from the viewpoints of basic science and clinical practic.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
