J.M. López-Millán Infantes , C. Coca-Gamito , A. Cámara-Faraig , E. Díaz-Infante , J.C. García Rubira
{"title":"Bloqueo del ganglio estrellado como tratamiento de la tormenta arrítmica: estudio observacional","authors":"J.M. López-Millán Infantes , C. Coca-Gamito , A. Cámara-Faraig , E. Díaz-Infante , J.C. García Rubira","doi":"10.1016/j.redar.2023.01.004","DOIUrl":null,"url":null,"abstract":"<div><h3>Introduction</h3><p>Arrhythmic storm is a life-threatening emergency with a high mortality rate. When acute conventional treatment is ineffective, a stellate ganglion block can contribute to the control of the arrhythmia by providing a visceral cervicothoracic sympathetic block. The objective of the study is to assess the effectiveness and safety of stellate ganglion blocks for the treatment of refractory arrhythmic storm.</p></div><div><h3>Method</h3><p>Follow-up of a cohort of patients with refractory arrhythmic storm that met the criteria for performing stellate ganglion blocks. The block was ultrasound-guided at C6-level using local anaesthetic and a steroid, left unilateral first, bilateral if no response, and followed by fluoroscopy-guided radiofrequency ablation at C7 if there was a favourable response but subsequent relapse.</p></div><div><h3>Results</h3><p>Seven patients were included, with a mortality rate during admission of 14.29%. Four patients received unilateral and three bilateral stellate ganglion blocks. Six were ablated and one of them had an implanted cardioverter-defibrillator. Arrhythmic storm was controlled temporarily beyond the effect of the local anaesthetic in all patients. Three underwent radiofrequency ablation and two underwent surgical thoracic sympathectomy. The only side effect was Horner's syndrome, which was observed in all cases after administering a stellate ganglion block with local anaesthetic. Two died after discharge and four are still at home, three of them without further admission due to ventricular events for more than two years.</p></div><div><h3>Conclusion</h3><p>An ultrasound-guided stellate ganglion block is an effective and safe technique in the treatment of refractory arrhythmic storm as a complement to the usual cardiological treatment.</p></div>","PeriodicalId":46479,"journal":{"name":"Revista Espanola de Anestesiologia y Reanimacion","volume":"71 1","pages":"Pages 1-7"},"PeriodicalIF":0.8000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Revista Espanola de Anestesiologia y Reanimacion","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S003493562300169X","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction
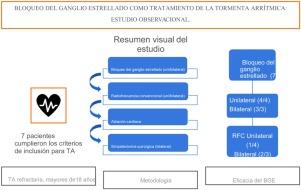
Arrhythmic storm is a life-threatening emergency with a high mortality rate. When acute conventional treatment is ineffective, a stellate ganglion block can contribute to the control of the arrhythmia by providing a visceral cervicothoracic sympathetic block. The objective of the study is to assess the effectiveness and safety of stellate ganglion blocks for the treatment of refractory arrhythmic storm.
Method
Follow-up of a cohort of patients with refractory arrhythmic storm that met the criteria for performing stellate ganglion blocks. The block was ultrasound-guided at C6-level using local anaesthetic and a steroid, left unilateral first, bilateral if no response, and followed by fluoroscopy-guided radiofrequency ablation at C7 if there was a favourable response but subsequent relapse.
Results
Seven patients were included, with a mortality rate during admission of 14.29%. Four patients received unilateral and three bilateral stellate ganglion blocks. Six were ablated and one of them had an implanted cardioverter-defibrillator. Arrhythmic storm was controlled temporarily beyond the effect of the local anaesthetic in all patients. Three underwent radiofrequency ablation and two underwent surgical thoracic sympathectomy. The only side effect was Horner's syndrome, which was observed in all cases after administering a stellate ganglion block with local anaesthetic. Two died after discharge and four are still at home, three of them without further admission due to ventricular events for more than two years.
Conclusion
An ultrasound-guided stellate ganglion block is an effective and safe technique in the treatment of refractory arrhythmic storm as a complement to the usual cardiological treatment.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
