{"title":"Heart failure drug classes and 30-day unplanned hospital readmission among patients with heart failure in Ethiopia.","authors":"Birhanu Ayenew, Prem Kumar, Adem Hussein, Yegoraw Gashaw, Mitaw Girma, Abdulmelik Ayalew, Beza Tadesse","doi":"10.1186/s40780-023-00320-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Drug therapy is a crucial aspect of heart failure management and has been shown to reduce morbidity and mortality in heart failure patients. However, the comparative effects of these drug classes on readmission rates have not been well studied. Therefore, the aim of this study was to examine the association between different classes of heart failure drugs and 30-day readmission rates in patients with heart failure.</p><p><strong>Method: </strong>A multicenter, hospital-based retrospective cohort design was employed and 572 randomly selected patients with heart failure were included. Data were entered in Epi-data version 4.6 and analyzed with STATA version 17. Kaplan-Meier and log-rank tests were used to estimate and compare survival time. A Cox proportional hazard model was utilized, employing both bi-variable and multi-variable analyses, to examine the effect of predictors on the timing of unplanned hospital readmissions. The strength of the association was assessed using an adjusted hazard ratio (aHR), and statistical significance was declared for p-values < 0.05 and a 95% confidence interval (CI).</p><p><strong>Results: </strong>In this study, a total of 151 (26.40%) heart failure patients were readmitted within 30 days of discharge. In the multivariate cox proportional hazards analysis being an age (> 65 year) (AHR: 2.34, 95%CI: 1.63, 3.37), rural in residency (AHR: 1.85, 95%CI: 1.07, 3.20), hospital stays > 7 Days (AHR: 3.68, 95%CI: 2.51,5.39), discharge with Diuretics (AHR: 2.37, 95%CI: 1.45, 3.86), and discharge with Beta-Blocker (AHR: 0.48, 95%CI: 0 0.34, 0.69) were identified as independent predictors of unplanned hospital readmission.</p><p><strong>Conclusion: </strong>Elderly patients, being in rural areas, longer hospital stays, and discharges of patients on diuretics and not on beta-blockers were independent predictors of unplanned hospital readmission. Therefore, working on these factors will help to reduce the hazard of unplanned hospital readmissions, improve patient outcomes, and increase the efficiency of heart failure management.</p>","PeriodicalId":16730,"journal":{"name":"Journal of Pharmaceutical Health Care and Sciences","volume":"9 1","pages":"49"},"PeriodicalIF":1.2000,"publicationDate":"2023-11-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10680257/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Pharmaceutical Health Care and Sciences","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40780-023-00320-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Drug therapy is a crucial aspect of heart failure management and has been shown to reduce morbidity and mortality in heart failure patients. However, the comparative effects of these drug classes on readmission rates have not been well studied. Therefore, the aim of this study was to examine the association between different classes of heart failure drugs and 30-day readmission rates in patients with heart failure.
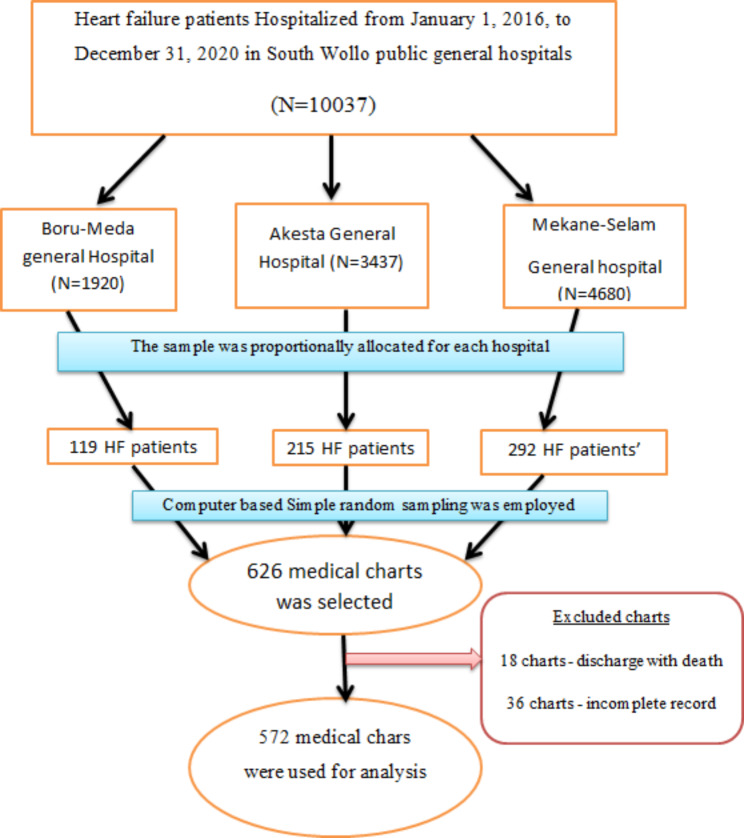
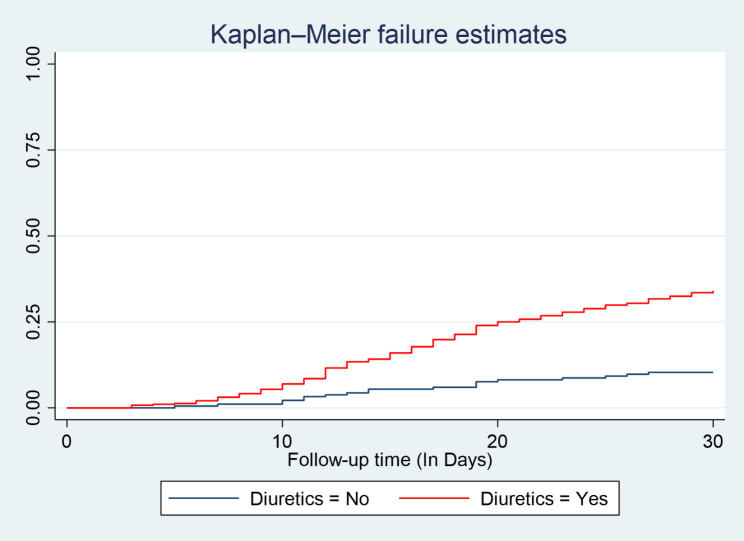
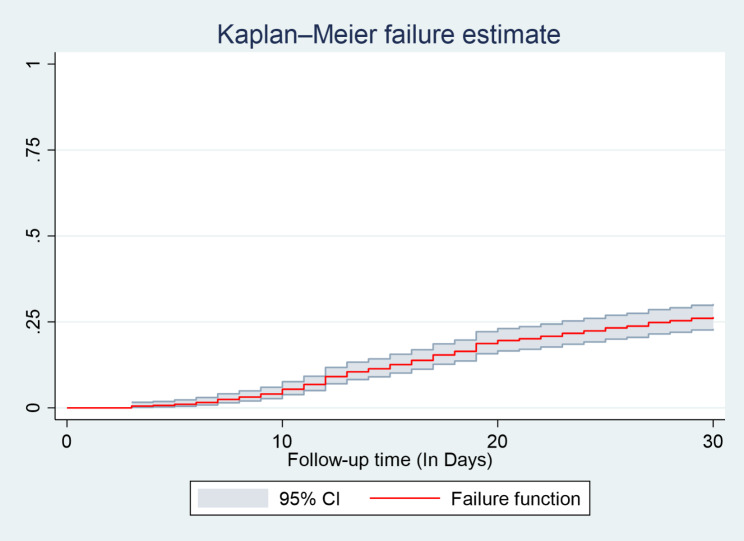
Method: A multicenter, hospital-based retrospective cohort design was employed and 572 randomly selected patients with heart failure were included. Data were entered in Epi-data version 4.6 and analyzed with STATA version 17. Kaplan-Meier and log-rank tests were used to estimate and compare survival time. A Cox proportional hazard model was utilized, employing both bi-variable and multi-variable analyses, to examine the effect of predictors on the timing of unplanned hospital readmissions. The strength of the association was assessed using an adjusted hazard ratio (aHR), and statistical significance was declared for p-values < 0.05 and a 95% confidence interval (CI).
Results: In this study, a total of 151 (26.40%) heart failure patients were readmitted within 30 days of discharge. In the multivariate cox proportional hazards analysis being an age (> 65 year) (AHR: 2.34, 95%CI: 1.63, 3.37), rural in residency (AHR: 1.85, 95%CI: 1.07, 3.20), hospital stays > 7 Days (AHR: 3.68, 95%CI: 2.51,5.39), discharge with Diuretics (AHR: 2.37, 95%CI: 1.45, 3.86), and discharge with Beta-Blocker (AHR: 0.48, 95%CI: 0 0.34, 0.69) were identified as independent predictors of unplanned hospital readmission.
Conclusion: Elderly patients, being in rural areas, longer hospital stays, and discharges of patients on diuretics and not on beta-blockers were independent predictors of unplanned hospital readmission. Therefore, working on these factors will help to reduce the hazard of unplanned hospital readmissions, improve patient outcomes, and increase the efficiency of heart failure management.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
