Janneke A C van Baar, Elena B Kostova, John Allotey, Shakila Thangaratinam, Javier R Zamora, Mercedes Bonet, Caron Rahn Kim, Lynne M Mofenson, Heinke Kunst, Asma Khalil, Elisabeth van Leeuwen, Julia Keijzer, Marije Strikwerda, Bethany Clark, Maxime Verschuuren, Arri Coomarasamy, Mariëtte Goddijn, Madelon van Wely
{"title":"COVID-19 in pregnant women: a systematic review and meta-analysis on the risk and prevalence of pregnancy loss.","authors":"Janneke A C van Baar, Elena B Kostova, John Allotey, Shakila Thangaratinam, Javier R Zamora, Mercedes Bonet, Caron Rahn Kim, Lynne M Mofenson, Heinke Kunst, Asma Khalil, Elisabeth van Leeuwen, Julia Keijzer, Marije Strikwerda, Bethany Clark, Maxime Verschuuren, Arri Coomarasamy, Mariëtte Goddijn, Madelon van Wely","doi":"10.1093/humupd/dmad030","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pregnant women infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) are more likely to experience preterm birth and their neonates are more likely to be stillborn or admitted to a neonatal unit. The World Health Organization declared in May 2023 an end to the coronavirus disease 2019 (COVID-19) pandemic as a global health emergency. However, pregnant women are still becoming infected with SARS-CoV-2 and there is limited information available regarding the effect of SARS-CoV-2 infection in early pregnancy on pregnancy outcomes.</p><p><strong>Objective and rationale: </strong>We conducted this systematic review to determine the prevalence of early pregnancy loss in women with SARS-Cov-2 infection and compare the risk to pregnant women without SARS-CoV-2 infection.</p><p><strong>Search methods: </strong>Our systematic review is based on a prospectively registered protocol. The search of PregCov19 consortium was supplemented with an extra electronic search specifically on pregnancy loss in pregnant women infected with SARS-CoV-2 up to 10 March 2023 in PubMed, Google Scholar, and LitCovid. We included retrospective and prospective studies of pregnant women with SARS-CoV-2 infection, provided that they contained information on pregnancy losses in the first and/or second trimester. Primary outcome was miscarriage defined as a pregnancy loss before 20 weeks of gestation, however, studies that reported loss up to 22 or 24 weeks were also included. Additionally, we report on studies that defined the pregnancy loss to occur at the first and/or second trimester of pregnancy without specifying gestational age, and for second trimester miscarriage only when the study presented stillbirths and/or foetal losses separately from miscarriages. Data were stratified into first and second trimester. Secondary outcomes were ectopic pregnancy (any extra-uterine pregnancy), and termination of pregnancy. At least three researchers independently extracted the data and assessed study quality. We calculated odds ratios (OR) and risk differences (RDs) with corresponding 95% CI and pooled the data using random effects meta-analysis. To estimate risk prevalence, we performed meta-analysis on proportions. Heterogeneity was assessed by I2.</p><p><strong>Outcomes: </strong>We included 120 studies comprising a total of 168 444 pregnant women with SARS-CoV-2 infection; of which 18 233 women were in their first or second trimester of pregnancy. Evidence level was considered to be of low to moderate certainty, mostly owing to selection bias. We did not find evidence of an association between SARS-CoV-2 infection and miscarriage (OR 1.10, 95% CI 0.81-1.48; I2 = 0.0%; RD 0.0012, 95% CI -0.0103 to 0.0127; I2 = 0%; 9 studies, 4439 women). Miscarriage occurred in 9.9% (95% CI 6.2-14.0%; I2 = 68%; 46 studies, 1797 women) of the women with SARS CoV-2 infection in their first trimester and in 1.2% (95% CI 0.3-2.4%; I2 = 34%; 33 studies; 3159 women) in the second trimester. The proportion of ectopic pregnancies in women with SARS-CoV-2 infection was 1.4% (95% CI 0.02-4.2%; I2 = 66%; 14 studies, 950 women). Termination of pregnancy occurred in 0.6% of the women (95% CI 0.01-1.6%; I2 = 79%; 39 studies; 1166 women).</p><p><strong>Wider implications: </strong>Our study found no indication that SARS-CoV-2 infection in the first or second trimester increases the risk of miscarriages. To provide better risk estimates, well-designed studies are needed that include pregnant women with and without SARS-CoV-2 infection at conception and early pregnancy and consider the association of clinical manifestation and severity of SARS-CoV-2 infection with pregnancy loss, as well as potential confounding factors such as previous pregnancy loss. For clinical practice, pregnant women should still be advised to take precautions to avoid risk of SARS-CoV-2 exposure and receive SARS-CoV-2 vaccination.</p>","PeriodicalId":55045,"journal":{"name":"Human Reproduction Update","volume":" ","pages":"133-152"},"PeriodicalIF":16.1000,"publicationDate":"2024-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10905512/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Human Reproduction Update","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/humupd/dmad030","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Pregnant women infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) are more likely to experience preterm birth and their neonates are more likely to be stillborn or admitted to a neonatal unit. The World Health Organization declared in May 2023 an end to the coronavirus disease 2019 (COVID-19) pandemic as a global health emergency. However, pregnant women are still becoming infected with SARS-CoV-2 and there is limited information available regarding the effect of SARS-CoV-2 infection in early pregnancy on pregnancy outcomes.
Objective and rationale: We conducted this systematic review to determine the prevalence of early pregnancy loss in women with SARS-Cov-2 infection and compare the risk to pregnant women without SARS-CoV-2 infection.
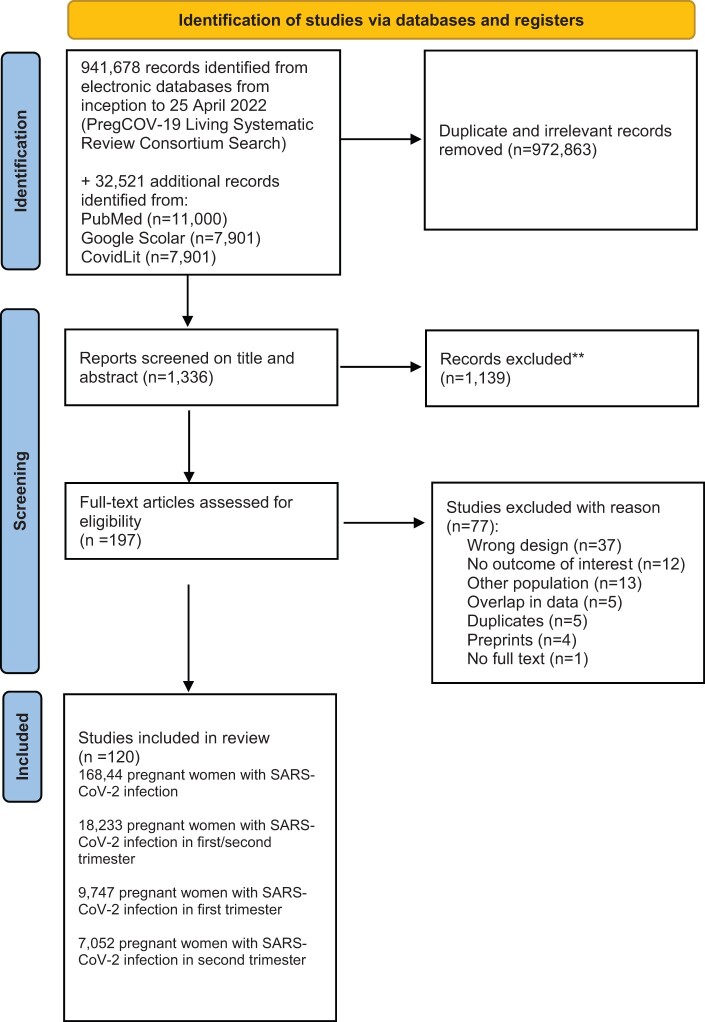
Search methods: Our systematic review is based on a prospectively registered protocol. The search of PregCov19 consortium was supplemented with an extra electronic search specifically on pregnancy loss in pregnant women infected with SARS-CoV-2 up to 10 March 2023 in PubMed, Google Scholar, and LitCovid. We included retrospective and prospective studies of pregnant women with SARS-CoV-2 infection, provided that they contained information on pregnancy losses in the first and/or second trimester. Primary outcome was miscarriage defined as a pregnancy loss before 20 weeks of gestation, however, studies that reported loss up to 22 or 24 weeks were also included. Additionally, we report on studies that defined the pregnancy loss to occur at the first and/or second trimester of pregnancy without specifying gestational age, and for second trimester miscarriage only when the study presented stillbirths and/or foetal losses separately from miscarriages. Data were stratified into first and second trimester. Secondary outcomes were ectopic pregnancy (any extra-uterine pregnancy), and termination of pregnancy. At least three researchers independently extracted the data and assessed study quality. We calculated odds ratios (OR) and risk differences (RDs) with corresponding 95% CI and pooled the data using random effects meta-analysis. To estimate risk prevalence, we performed meta-analysis on proportions. Heterogeneity was assessed by I2.
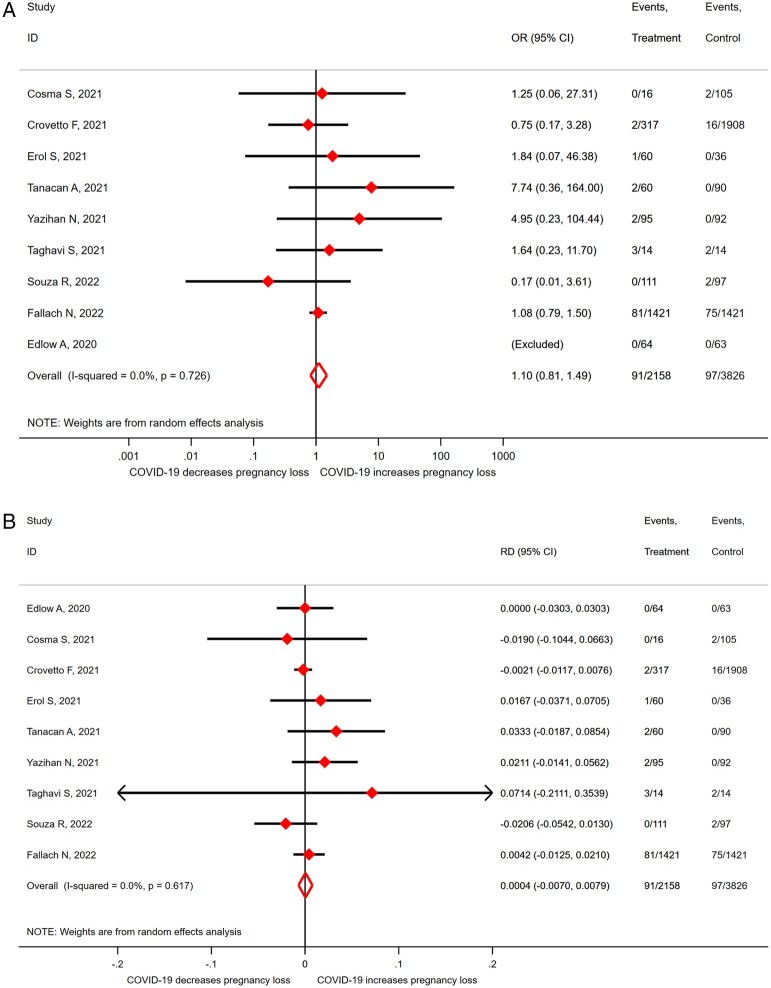
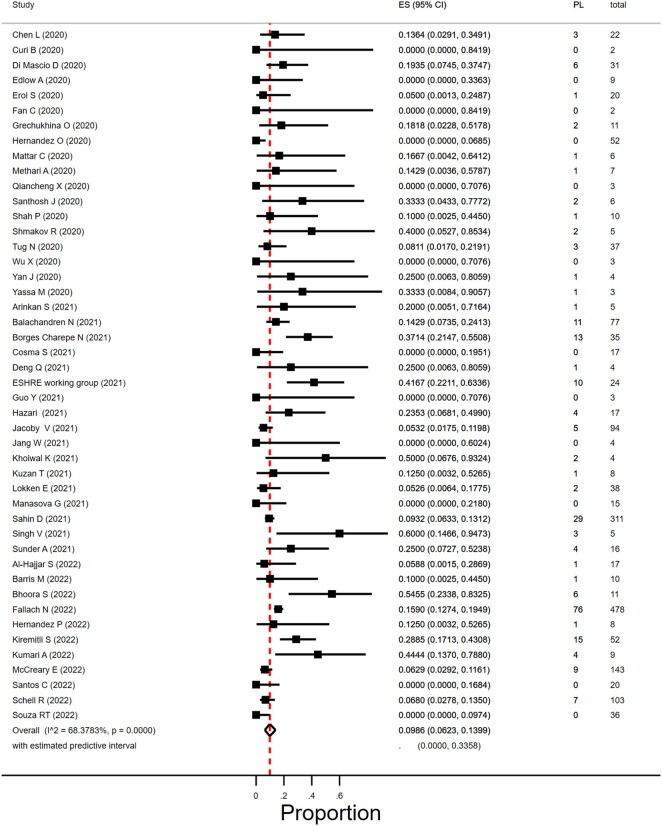
Outcomes: We included 120 studies comprising a total of 168 444 pregnant women with SARS-CoV-2 infection; of which 18 233 women were in their first or second trimester of pregnancy. Evidence level was considered to be of low to moderate certainty, mostly owing to selection bias. We did not find evidence of an association between SARS-CoV-2 infection and miscarriage (OR 1.10, 95% CI 0.81-1.48; I2 = 0.0%; RD 0.0012, 95% CI -0.0103 to 0.0127; I2 = 0%; 9 studies, 4439 women). Miscarriage occurred in 9.9% (95% CI 6.2-14.0%; I2 = 68%; 46 studies, 1797 women) of the women with SARS CoV-2 infection in their first trimester and in 1.2% (95% CI 0.3-2.4%; I2 = 34%; 33 studies; 3159 women) in the second trimester. The proportion of ectopic pregnancies in women with SARS-CoV-2 infection was 1.4% (95% CI 0.02-4.2%; I2 = 66%; 14 studies, 950 women). Termination of pregnancy occurred in 0.6% of the women (95% CI 0.01-1.6%; I2 = 79%; 39 studies; 1166 women).
Wider implications: Our study found no indication that SARS-CoV-2 infection in the first or second trimester increases the risk of miscarriages. To provide better risk estimates, well-designed studies are needed that include pregnant women with and without SARS-CoV-2 infection at conception and early pregnancy and consider the association of clinical manifestation and severity of SARS-CoV-2 infection with pregnancy loss, as well as potential confounding factors such as previous pregnancy loss. For clinical practice, pregnant women should still be advised to take precautions to avoid risk of SARS-CoV-2 exposure and receive SARS-CoV-2 vaccination.
期刊介绍:
Human Reproduction Update is the leading journal in its field, boasting a Journal Impact FactorTM of 13.3 and ranked first in Obstetrics & Gynecology and Reproductive Biology (Source: Journal Citation ReportsTM from Clarivate, 2023). It specializes in publishing comprehensive and systematic review articles covering various aspects of human reproductive physiology and medicine.
The journal prioritizes basic, transitional, and clinical topics related to reproduction, encompassing areas such as andrology, embryology, infertility, gynaecology, pregnancy, reproductive endocrinology, reproductive epidemiology, reproductive genetics, reproductive immunology, and reproductive oncology. Human Reproduction Update is published on behalf of the European Society of Human Reproduction and Embryology (ESHRE), maintaining the highest scientific and editorial standards.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
