Facilitators and barriers to implementation of a patient and staff reported measure for screening of palliative concerns of patients with heart failure: a qualitative analysis using the Consolidated Framework for Implementation Research.
{"title":"Facilitators and barriers to implementation of a patient and staff reported measure for screening of palliative concerns of patients with heart failure: a qualitative analysis using the Consolidated Framework for Implementation Research.","authors":"Shirlyn Hui-Shan Neo, Jasmine Yun-Ting Tan, Elaine Swee-Ling Ng, Sungwon Yoon","doi":"10.1177/26323524231214814","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Screening patients with patient-reported outcome measures allows identification of palliative care concerns. The Integrated Palliative Care Outcome Scale (IPOS) was developed in the United Kingdom for this purpose. Tools developed in another setting might not be readily usable locally. We previously evaluated the validity and reliability of the IPOS in our cardiology setting. However, it remains uncertain what factors would influence the subsequent implementation of IPOS for routine screening of patients with advanced heart failure in future practice.</p><p><strong>Objectives: </strong>This study aimed to identify the factors that could affect the IPOS implementation for patients with advanced heart failure.</p><p><strong>Design: </strong>This was a qualitative study conducted at the National Heart Centre Singapore.</p><p><strong>Methods: </strong>Patients with advanced heart failure who participated in our previous IPOS validation study were purposively recruited for semi-structured interviews. Healthcare workers caring for these patients and involved in the testing of the IPOS tool were also invited for interviews. The interviews were analyzed thematically and mapped to the Consolidated Framework for Implementation Research (CFIR).</p><p><strong>Results: </strong>Our analysis identified six potential facilitators and six potential barriers to implementation across five major domains of the CFIR (intervention characteristics, inner setting, outer setting, individual characteristics, and process). Facilitators include: (i) perception of utility, (ii) perception of minimal complexity, (iii) perception of relatability, (iv) conducive culture, (v) dedicated resources, and (vi) advocates for implementation. Barriers include: (i) need for adaptation, (ii) mindsets/role strains, (iii) resource constraints, (iv) cultural concerns, (v) individual needs, and (vi) change process.</p><p><strong>Conclusion: </strong>Institutions could focus on cultivating appropriate perceptions and conducive cultures, providing dedicated resources for implementation and introducing facilitators to advocate for implementation. Adaptation of IPOS to suit workflows and individual needs, consideration of change processes, and systemic changes to alleviate cultural, resource, and staff role strains would improve IPOS uptake during actual implementation in clinical services.</p><p><strong>Trial registration: </strong>Not applicable.</p>","PeriodicalId":36693,"journal":{"name":"Palliative Care and Social Practice","volume":"17 ","pages":"26323524231214814"},"PeriodicalIF":2.2000,"publicationDate":"2023-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10693212/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Palliative Care and Social Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26323524231214814","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Screening patients with patient-reported outcome measures allows identification of palliative care concerns. The Integrated Palliative Care Outcome Scale (IPOS) was developed in the United Kingdom for this purpose. Tools developed in another setting might not be readily usable locally. We previously evaluated the validity and reliability of the IPOS in our cardiology setting. However, it remains uncertain what factors would influence the subsequent implementation of IPOS for routine screening of patients with advanced heart failure in future practice.
Objectives: This study aimed to identify the factors that could affect the IPOS implementation for patients with advanced heart failure.
Design: This was a qualitative study conducted at the National Heart Centre Singapore.
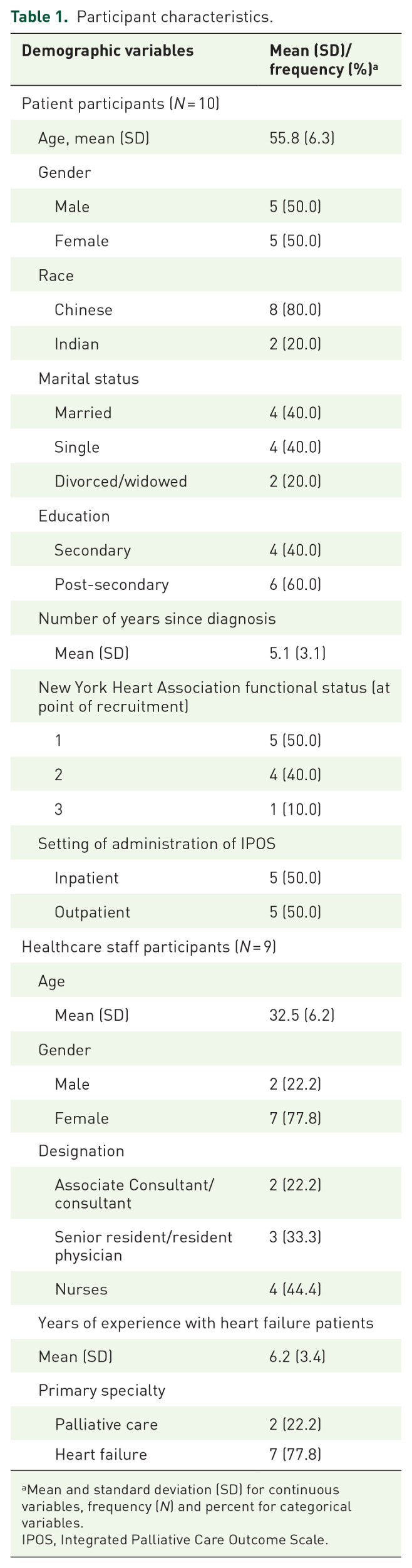
Methods: Patients with advanced heart failure who participated in our previous IPOS validation study were purposively recruited for semi-structured interviews. Healthcare workers caring for these patients and involved in the testing of the IPOS tool were also invited for interviews. The interviews were analyzed thematically and mapped to the Consolidated Framework for Implementation Research (CFIR).
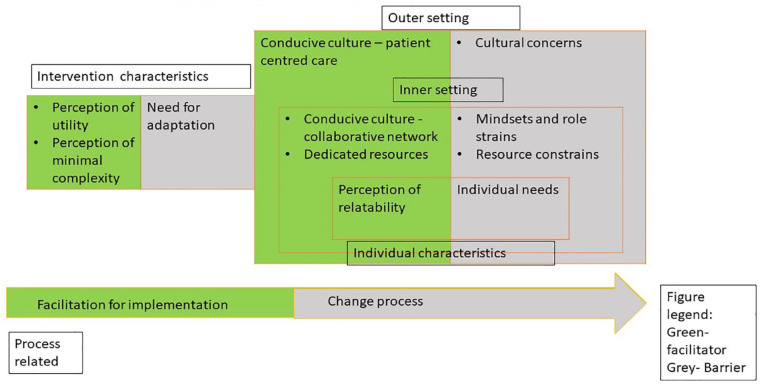
Results: Our analysis identified six potential facilitators and six potential barriers to implementation across five major domains of the CFIR (intervention characteristics, inner setting, outer setting, individual characteristics, and process). Facilitators include: (i) perception of utility, (ii) perception of minimal complexity, (iii) perception of relatability, (iv) conducive culture, (v) dedicated resources, and (vi) advocates for implementation. Barriers include: (i) need for adaptation, (ii) mindsets/role strains, (iii) resource constraints, (iv) cultural concerns, (v) individual needs, and (vi) change process.
Conclusion: Institutions could focus on cultivating appropriate perceptions and conducive cultures, providing dedicated resources for implementation and introducing facilitators to advocate for implementation. Adaptation of IPOS to suit workflows and individual needs, consideration of change processes, and systemic changes to alleviate cultural, resource, and staff role strains would improve IPOS uptake during actual implementation in clinical services.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
