Yibo Ma, Lanyan Guo, Huani Pang, Qun Yan, Jie Li, Miaoyang Hu, Fu Yi
{"title":"Failure of intravenous nifekalant cardioversion as an independent predictor for persistent atrial fibrillation recurrence after catheter ablation.","authors":"Yibo Ma, Lanyan Guo, Huani Pang, Qun Yan, Jie Li, Miaoyang Hu, Fu Yi","doi":"10.1007/s10840-023-01713-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Nifekalant is a class III antiarrhythmic drug that exerts antiarrhythmic effects by inhibiting rapid rectifying potassium channels and extending the effective refractory period of cardiomyocytes. It has a high success rate in converting atrial fibrillation (AF) to sinus rhythm. Whether the failure of intravenous nifekalant cardioversion is an independent predictor for persistent AF recurrence after catheter ablation has not been reported.</p><p><strong>Methods: </strong>A total of 92 patients with drug-refractory persistent AF were retrospectively enrolled. After all ablations, intravenous nifekalant was administrated. Patients were assigned to the success group (group 1) and failure group (group 2) based on nifekalant cardioversion results and followed for 12 months to note any episode of atrial arrhythmia recurrence.</p><p><strong>Results: </strong>Each group included 46 patients. After 12 months of follow-up, nine (19.6%) patients from group 1 and 23 (50.0%) patients from group 2 had a recurrence of atrial tachyarrhythmia (P = 0.002). AF duration and type 2 diabetes were strongly associated with failure of intravenous nifekalant cardioversion. Univariable Cox proportional hazard regression showed that failure of intravenous nifekalant cardioversion, AF duration, and type 2 diabetes were potential risk factors. Multivariable Cox proportional hazard regression showed that failure of nifekalant cardioversion was statistically associated with AF recurrence (adjusted RR = 2.257, 95% CI: 1.006-5.066, P = 0.048). Failure of intravenous nifekalant cardioversion could bring a positive effect on the prognostic differentiation when added into the multivariable model (0.767 ± 0.042 vs. 0.774 ± 0.045, P = 0.025).</p><p><strong>Conclusion: </strong>Failure of nifekalant cardioversion is an independent predictor for persistent AF recurrence after catheter ablation.</p>","PeriodicalId":16202,"journal":{"name":"Journal of Interventional Cardiac Electrophysiology","volume":" ","pages":"1161-1171"},"PeriodicalIF":2.6000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Interventional Cardiac Electrophysiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10840-023-01713-7","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/12/5 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: Nifekalant is a class III antiarrhythmic drug that exerts antiarrhythmic effects by inhibiting rapid rectifying potassium channels and extending the effective refractory period of cardiomyocytes. It has a high success rate in converting atrial fibrillation (AF) to sinus rhythm. Whether the failure of intravenous nifekalant cardioversion is an independent predictor for persistent AF recurrence after catheter ablation has not been reported.
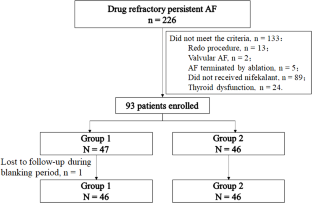
Methods: A total of 92 patients with drug-refractory persistent AF were retrospectively enrolled. After all ablations, intravenous nifekalant was administrated. Patients were assigned to the success group (group 1) and failure group (group 2) based on nifekalant cardioversion results and followed for 12 months to note any episode of atrial arrhythmia recurrence.
Results: Each group included 46 patients. After 12 months of follow-up, nine (19.6%) patients from group 1 and 23 (50.0%) patients from group 2 had a recurrence of atrial tachyarrhythmia (P = 0.002). AF duration and type 2 diabetes were strongly associated with failure of intravenous nifekalant cardioversion. Univariable Cox proportional hazard regression showed that failure of intravenous nifekalant cardioversion, AF duration, and type 2 diabetes were potential risk factors. Multivariable Cox proportional hazard regression showed that failure of nifekalant cardioversion was statistically associated with AF recurrence (adjusted RR = 2.257, 95% CI: 1.006-5.066, P = 0.048). Failure of intravenous nifekalant cardioversion could bring a positive effect on the prognostic differentiation when added into the multivariable model (0.767 ± 0.042 vs. 0.774 ± 0.045, P = 0.025).
Conclusion: Failure of nifekalant cardioversion is an independent predictor for persistent AF recurrence after catheter ablation.
期刊介绍:
The Journal of Interventional Cardiac Electrophysiology is an international publication devoted to fostering research in and development of interventional techniques and therapies for the management of cardiac arrhythmias. It is designed primarily to present original research studies and scholarly scientific reviews of basic and applied science and clinical research in this field. The Journal will adopt a multidisciplinary approach to link physical, experimental, and clinical sciences as applied to the development of and practice in interventional electrophysiology. The Journal will examine techniques ranging from molecular, chemical and pharmacologic therapies to device and ablation technology. Accordingly, original research in clinical, epidemiologic and basic science arenas will be considered for publication. Applied engineering or physical science studies pertaining to interventional electrophysiology will be encouraged. The Journal is committed to providing comprehensive and detailed treatment of major interventional therapies and innovative techniques in a structured and clinically relevant manner. It is directed at clinical practitioners and investigators in the rapidly growing field of interventional electrophysiology. The editorial staff and board reflect this bias and include noted international experts in this area with a wealth of expertise in basic and clinical investigation. Peer review of all submissions, conflict of interest guidelines and periodic editorial board review of all Journal policies have been established.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
