{"title":"A 63-year-old woman with parietal scalp surface rugged","authors":"Zhiwei Shen, Siqi Tao","doi":"10.1111/bpa.13224","DOIUrl":null,"url":null,"abstract":"<p>A 63-year-old woman presented with a 2-month history of a rugged surface on the left parietal scalp. She reported slight pain when pressing the skin over the irregular area. Computed tomography (CT) showed mottling and small patchy destruction of the left parietal bone. Cranial contrast magnetic resonance imaging (MRI) revealed a homogeneously-enhanced, en plaque mass, measuring 59 × 22 mm. The MRI also showed that the mass had infiltrated the parietal bone, and the dural tail sign was present (Figure 1). Blood tests ruled out anemia (hemoglobin 10.6 g/dL), hypercalcemia (serum calcium: 2.25 mmol/L), and renal insufficiency (serum creatinine: 54 μmol/L). She denied having headaches, vomiting, epileptic seizures, and paresthesia. No other lesions were found during physical examination or imaging studies. On the basis of the radiological features of the lesion, en plaque meningioma was highly suspected, and the patient was advised to undergo tumor resection. Intraoperatively, the tumor was located in the epidural space and was completely resected via a left-sided parietal approach. The invaded bone was excised, and titanium mesh was used to restore the cranial bone defect. Postoperatively, the patient had no neurological deficits and was discharged on postoperative day 5 (Box 1).</p><p>Hematoxylin and eosin (H&E) staining showed a large number of cells with eccentrically located nuclei and prominent large nucleoli resembling plasma cells in the parietal lobe mass (Figure 2A). Immunohistochemical staining revealed tumor cells positive for cluster of differentiation (CD) 56 (Figure 2B), multiple myeloma oncogene 1 (MuM-1) (Figure 2C), lambda immunoglobulin light chains (Figure 2D), CD79a, but negative for side-to-side kappa immunoglobulin light chains (Figure 2E). The Ki-67 proliferation index was 15% (Figure 2F). In situ hybridization for Epstein–Barr virus encoded RNA was negative. Additionally, the tumor was negative for CD138, CD38, CD19, CD30, and cyclin D1 with immunohistochemical staining.</p><p>Plasma cell neoplasm.</p><p>The unexpected pathological diagnosis prompted a referral to hematology. In the hematology department, our patient underwent further evaluation, including urinalysis for Bence-Jones protein, PET, and bone marrow examination. The results of immunoglobulin testing were normal, and bone marrow examination revealed that the plasma cell percentage was 8.5%. Postoperative PET/CT revealed postoperative changes after resection of the left parietal tumor; no significant increase in glucose metabolism was observed in the whole-body images. All of above supported the diagnosis of plasmacytoma.</p><p>According to the International Consensus Classification of mature lymphoid neoplasms, plasmacytoma is defined as a localized neoplasm of clonal plasma cells without evidence of multiple myeloma. The diagnostic criteria are as follows: (1) biopsy-proven clonal plasma cell neoplasm of bone or extramedullary site; (2) no clonal B cells; (3) no other lesions on physical examination or radiographic studies; (4) no end-organ damage (hypercalcemia, renal insufficiency, anemia or bone lesions) due to the plasma cell neoplasm; and (5) minimal bone marrow involvement (< 10% clonal plasma cells) [<span>1</span>]. The diagnosis of plasmacytoma depends mainly on bone marrow examination, whole-body CT scan or fluordeoxyglucose positron emission tomography (PET)/CT, and serum monoclonal immunoglobulin assessment [<span>2</span>]. Skull plasmacytoma belongs to the category of localized plasma cell neoplasm of bone, which is characterized by skull bone destruction and local soft tissue mass formation. Intracranial plasmacytoma that radiologically mimic the appearance of meningioma, as described in our case, are uncommon.</p><p>Typically, tumors on the parietal surface comprise meningiomas, metastatic carcinoma, and plasmacytoma. These lesions are contrast-enhanced on MRI and may be associated with adjacent bony erosions. In our patient, meningioma was considered most likely because of the presence of the dural tail sign and the high incidence on the parietal surface. However, it should be noted that meningiomas usually invade adjacent bone slowly and rarely cause osteolytic changes. Metastatic carcinoma usually shows multiple lesions with punched-out margins. Plasmacytoma may present as osteolytic lesions on CT and strongly-enhanced lesions on T1-weighted MRI [<span>3</span>].</p><p>Histopathological identification is necessary for the diagnosis and subsequent treatment of a plasmacytoma. In our case, a resection approach was selected as a meningioma with a mass effect was highly suspected. Surprisingly, a large number of cells resembling plasma cells were found in pathological sections. Although the sample from our patient tested negative for CD138 and CD38, which is unusual in plasma cell neoplasm, the absence of other lesions, and the presence of eccentric nuclei, lambda immunoglobulin light chain restriction, and positive staining for CD79a, CD56, and MuM-1, support the diagnosis of plasmacytoma. The patient was subsequently treated with radiotherapy. During the 1-year follow-up after surgery, she remained stable regarding head imaging, and she reported good overall health.</p><p>In summary, we report a rare case showing that plasmacytoma can occur intracranially and mimic a meningiomas in imaging. If plasmacytoma had been suspected radiologically, a biopsy would have been more appropriate as a first intervention. Therefore, rare conditions, such as those described in this case, should be adequately considered by neurosurgeons and neuroradiologists.</p><p>Zhiwei Shen collected clinical data and drafted the manuscript. Siqi Tao performed and interpreted the histopathology. Both authors have read and approved the final version.</p><p>The authors have declared no conflicts of interest for this article.</p><p>The study was approved by the ethics committee of Second Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, China, and was conducted in full compliance with all principles of the Helsinki Declaration.</p>","PeriodicalId":9290,"journal":{"name":"Brain Pathology","volume":"34 2","pages":""},"PeriodicalIF":6.2000,"publicationDate":"2023-12-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/bpa.13224","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brain Pathology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/bpa.13224","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
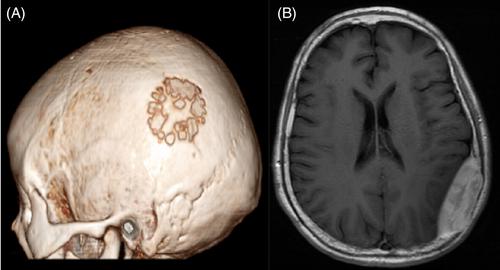
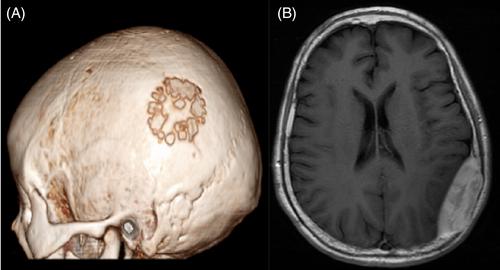
A 63-year-old woman presented with a 2-month history of a rugged surface on the left parietal scalp. She reported slight pain when pressing the skin over the irregular area. Computed tomography (CT) showed mottling and small patchy destruction of the left parietal bone. Cranial contrast magnetic resonance imaging (MRI) revealed a homogeneously-enhanced, en plaque mass, measuring 59 × 22 mm. The MRI also showed that the mass had infiltrated the parietal bone, and the dural tail sign was present (Figure 1). Blood tests ruled out anemia (hemoglobin 10.6 g/dL), hypercalcemia (serum calcium: 2.25 mmol/L), and renal insufficiency (serum creatinine: 54 μmol/L). She denied having headaches, vomiting, epileptic seizures, and paresthesia. No other lesions were found during physical examination or imaging studies. On the basis of the radiological features of the lesion, en plaque meningioma was highly suspected, and the patient was advised to undergo tumor resection. Intraoperatively, the tumor was located in the epidural space and was completely resected via a left-sided parietal approach. The invaded bone was excised, and titanium mesh was used to restore the cranial bone defect. Postoperatively, the patient had no neurological deficits and was discharged on postoperative day 5 (Box 1).
Hematoxylin and eosin (H&E) staining showed a large number of cells with eccentrically located nuclei and prominent large nucleoli resembling plasma cells in the parietal lobe mass (Figure 2A). Immunohistochemical staining revealed tumor cells positive for cluster of differentiation (CD) 56 (Figure 2B), multiple myeloma oncogene 1 (MuM-1) (Figure 2C), lambda immunoglobulin light chains (Figure 2D), CD79a, but negative for side-to-side kappa immunoglobulin light chains (Figure 2E). The Ki-67 proliferation index was 15% (Figure 2F). In situ hybridization for Epstein–Barr virus encoded RNA was negative. Additionally, the tumor was negative for CD138, CD38, CD19, CD30, and cyclin D1 with immunohistochemical staining.
Plasma cell neoplasm.
The unexpected pathological diagnosis prompted a referral to hematology. In the hematology department, our patient underwent further evaluation, including urinalysis for Bence-Jones protein, PET, and bone marrow examination. The results of immunoglobulin testing were normal, and bone marrow examination revealed that the plasma cell percentage was 8.5%. Postoperative PET/CT revealed postoperative changes after resection of the left parietal tumor; no significant increase in glucose metabolism was observed in the whole-body images. All of above supported the diagnosis of plasmacytoma.
According to the International Consensus Classification of mature lymphoid neoplasms, plasmacytoma is defined as a localized neoplasm of clonal plasma cells without evidence of multiple myeloma. The diagnostic criteria are as follows: (1) biopsy-proven clonal plasma cell neoplasm of bone or extramedullary site; (2) no clonal B cells; (3) no other lesions on physical examination or radiographic studies; (4) no end-organ damage (hypercalcemia, renal insufficiency, anemia or bone lesions) due to the plasma cell neoplasm; and (5) minimal bone marrow involvement (< 10% clonal plasma cells) [1]. The diagnosis of plasmacytoma depends mainly on bone marrow examination, whole-body CT scan or fluordeoxyglucose positron emission tomography (PET)/CT, and serum monoclonal immunoglobulin assessment [2]. Skull plasmacytoma belongs to the category of localized plasma cell neoplasm of bone, which is characterized by skull bone destruction and local soft tissue mass formation. Intracranial plasmacytoma that radiologically mimic the appearance of meningioma, as described in our case, are uncommon.
Typically, tumors on the parietal surface comprise meningiomas, metastatic carcinoma, and plasmacytoma. These lesions are contrast-enhanced on MRI and may be associated with adjacent bony erosions. In our patient, meningioma was considered most likely because of the presence of the dural tail sign and the high incidence on the parietal surface. However, it should be noted that meningiomas usually invade adjacent bone slowly and rarely cause osteolytic changes. Metastatic carcinoma usually shows multiple lesions with punched-out margins. Plasmacytoma may present as osteolytic lesions on CT and strongly-enhanced lesions on T1-weighted MRI [3].
Histopathological identification is necessary for the diagnosis and subsequent treatment of a plasmacytoma. In our case, a resection approach was selected as a meningioma with a mass effect was highly suspected. Surprisingly, a large number of cells resembling plasma cells were found in pathological sections. Although the sample from our patient tested negative for CD138 and CD38, which is unusual in plasma cell neoplasm, the absence of other lesions, and the presence of eccentric nuclei, lambda immunoglobulin light chain restriction, and positive staining for CD79a, CD56, and MuM-1, support the diagnosis of plasmacytoma. The patient was subsequently treated with radiotherapy. During the 1-year follow-up after surgery, she remained stable regarding head imaging, and she reported good overall health.
In summary, we report a rare case showing that plasmacytoma can occur intracranially and mimic a meningiomas in imaging. If plasmacytoma had been suspected radiologically, a biopsy would have been more appropriate as a first intervention. Therefore, rare conditions, such as those described in this case, should be adequately considered by neurosurgeons and neuroradiologists.
Zhiwei Shen collected clinical data and drafted the manuscript. Siqi Tao performed and interpreted the histopathology. Both authors have read and approved the final version.
The authors have declared no conflicts of interest for this article.
The study was approved by the ethics committee of Second Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, China, and was conducted in full compliance with all principles of the Helsinki Declaration.
期刊介绍:
Brain Pathology is the journal of choice for biomedical scientists investigating diseases of the nervous system. The official journal of the International Society of Neuropathology, Brain Pathology is a peer-reviewed quarterly publication that includes original research, review articles and symposia focuses on the pathogenesis of neurological disease.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
