Increasing Incremental Burden of Surgical Bleeding Associated with Multiple Comorbidities as Measured by the Elixhauser Comorbidity Index: A Retrospective Database Analysis.
Mosadoluwa Afolabi, Stephen S Johnston, Pranjal Tewari, Walter A Danker
{"title":"Increasing Incremental Burden of Surgical Bleeding Associated with Multiple Comorbidities as Measured by the Elixhauser Comorbidity Index: A Retrospective Database Analysis.","authors":"Mosadoluwa Afolabi, Stephen S Johnston, Pranjal Tewari, Walter A Danker","doi":"10.2147/MDER.S434779","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Disruptive bleeding can complicate surgical procedures, increasing resource use, and impacting patients' well-being. This study aims to elucidate the impact of comorbidity on the risk of disruptive surgical-related bleeding and selected transfusion-associated complications, as well as the incremental cost of such bleeding.</p><p><strong>Patients and methods: </strong>This retrospective analysis of the Premier Healthcare Database included patients who were age ≥18 years and who had a procedure of interest between 1-Jan-2019-31-Dec-2019: cholecystectomy, coronary artery bypass grafting, cystectomy, hepatectomy, hysterectomy, pancreatectomy, peripheral vascular, thoracic, and valve procedures (first=index). The Elixhauser comorbidity index was assessed on index date and patients were grouped by cumulative comorbidity score (0, 1, 2, 3, 4, 5, ≥6). Outcomes, all measured as in-hospital during index, included bleeding (diagnosis and/or intervention for bleeding), transfusion-associated complications (diagnosis of infection, acute renal failure, or vascular events), and incremental total hospital costs associated with bleeding. Multivariable generalized linear models were used to examine the association of comorbidity/bleeding with outcomes.</p><p><strong>Results: </strong>Of the 304,074 patients included, 7% experienced bleeding. The Elixhauser scores were distributed as follows: 0=29%, 1=23%, 2=18%, 3=12%, 4=8%, 5=5%, ≥6=5%. Odds of bleeding significantly increased with Elixhauser score: 1 comorbidity vs 0 (odds ratio [OR] =1.30, 95% confidence interval [95% CI] =1.19-1.43), and this trend continued to surge (≥6 comorbidities [OR=3.22, 95% CI=2.94-3.53]). Similarly, the odds of transfusion-associated complications significantly increased with comorbidities score: 1 comorbidity vs 0 (OR=2.14, 95% CI=1.88-2.34), ≥6 comorbidities vs 0 (OR=12.37, 95% CI=10.80-14.16). The incremental cost of bleeding also increased with comorbidities score; per-patient costs with and without bleeding were $18,132 vs $13,190, p < 0.001 among patients with 0 comorbidities and $28,952 vs $19,623, p < 0.001 among patients with ≥6 comorbidities.</p><p><strong>Conclusion: </strong>Higher comorbidity burden was associated with significant increases in the risk of surgical bleeding, subsequent transfusion-related complications, and incremental cost burden of bleeding.</p>","PeriodicalId":47140,"journal":{"name":"Medical Devices-Evidence and Research","volume":"16 ","pages":"237-249"},"PeriodicalIF":1.5000,"publicationDate":"2023-12-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10706582/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical Devices-Evidence and Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/MDER.S434779","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ENGINEERING, BIOMEDICAL","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Disruptive bleeding can complicate surgical procedures, increasing resource use, and impacting patients' well-being. This study aims to elucidate the impact of comorbidity on the risk of disruptive surgical-related bleeding and selected transfusion-associated complications, as well as the incremental cost of such bleeding.
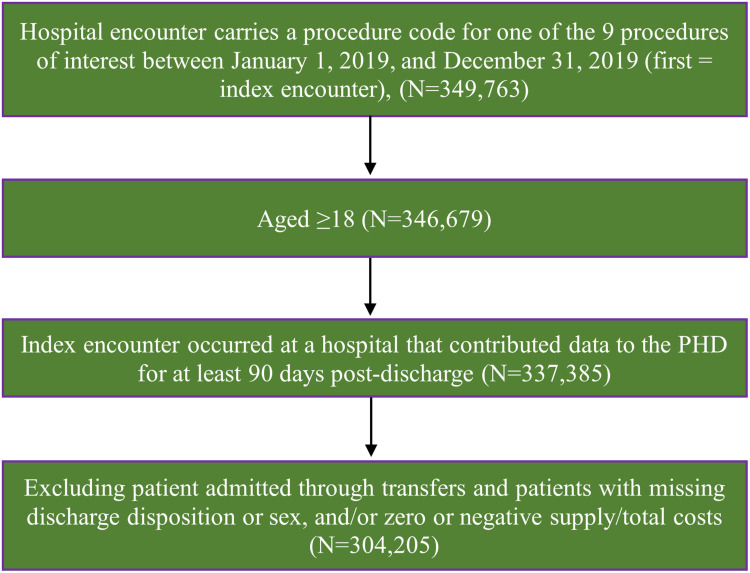
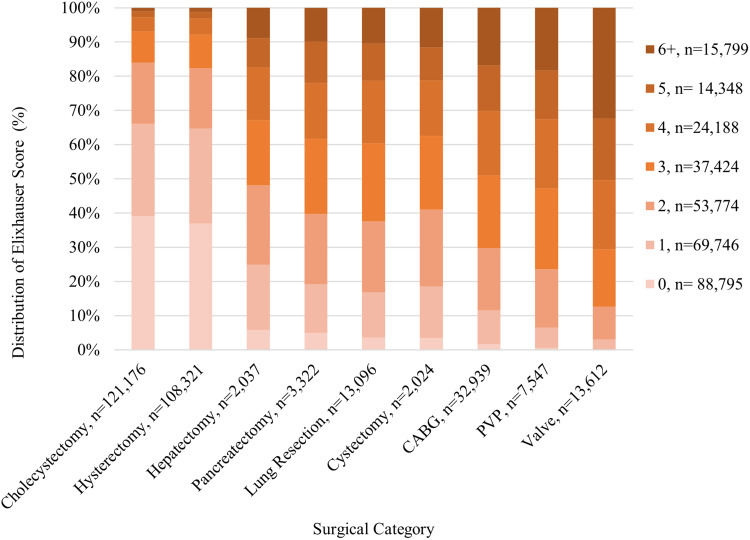
Patients and methods: This retrospective analysis of the Premier Healthcare Database included patients who were age ≥18 years and who had a procedure of interest between 1-Jan-2019-31-Dec-2019: cholecystectomy, coronary artery bypass grafting, cystectomy, hepatectomy, hysterectomy, pancreatectomy, peripheral vascular, thoracic, and valve procedures (first=index). The Elixhauser comorbidity index was assessed on index date and patients were grouped by cumulative comorbidity score (0, 1, 2, 3, 4, 5, ≥6). Outcomes, all measured as in-hospital during index, included bleeding (diagnosis and/or intervention for bleeding), transfusion-associated complications (diagnosis of infection, acute renal failure, or vascular events), and incremental total hospital costs associated with bleeding. Multivariable generalized linear models were used to examine the association of comorbidity/bleeding with outcomes.
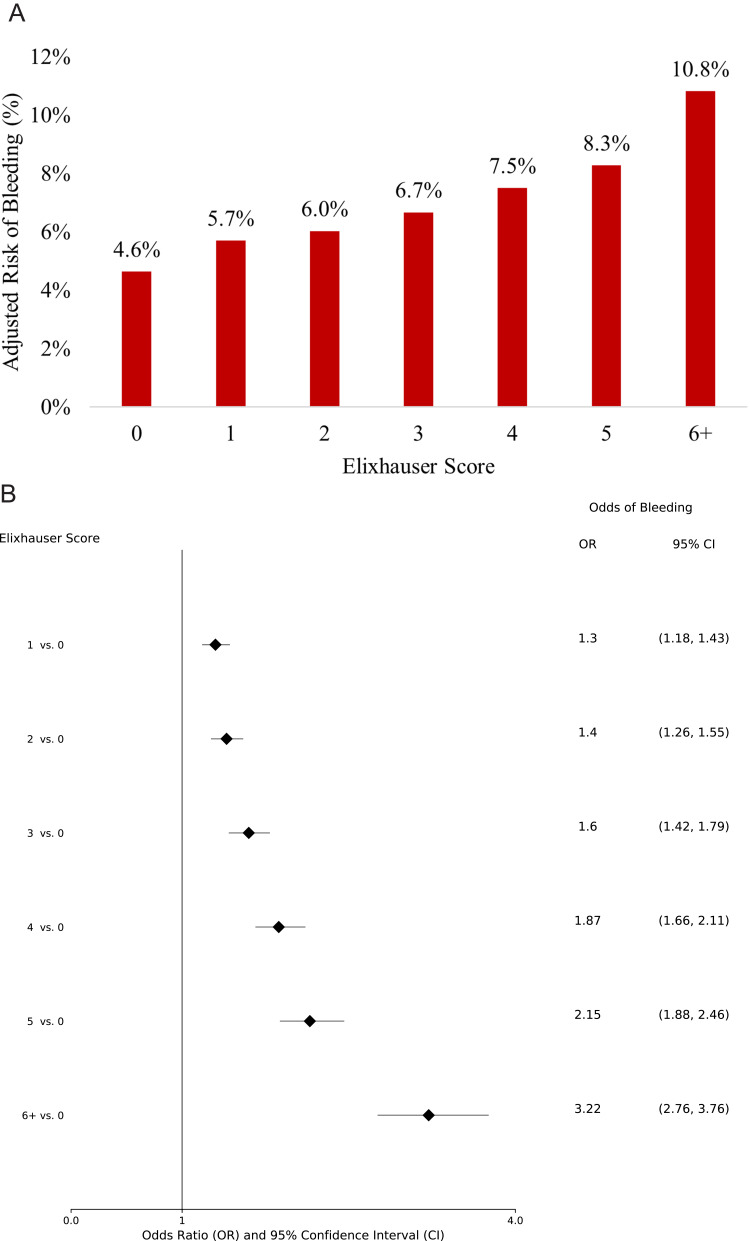
Results: Of the 304,074 patients included, 7% experienced bleeding. The Elixhauser scores were distributed as follows: 0=29%, 1=23%, 2=18%, 3=12%, 4=8%, 5=5%, ≥6=5%. Odds of bleeding significantly increased with Elixhauser score: 1 comorbidity vs 0 (odds ratio [OR] =1.30, 95% confidence interval [95% CI] =1.19-1.43), and this trend continued to surge (≥6 comorbidities [OR=3.22, 95% CI=2.94-3.53]). Similarly, the odds of transfusion-associated complications significantly increased with comorbidities score: 1 comorbidity vs 0 (OR=2.14, 95% CI=1.88-2.34), ≥6 comorbidities vs 0 (OR=12.37, 95% CI=10.80-14.16). The incremental cost of bleeding also increased with comorbidities score; per-patient costs with and without bleeding were $18,132 vs $13,190, p < 0.001 among patients with 0 comorbidities and $28,952 vs $19,623, p < 0.001 among patients with ≥6 comorbidities.
Conclusion: Higher comorbidity burden was associated with significant increases in the risk of surgical bleeding, subsequent transfusion-related complications, and incremental cost burden of bleeding.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
