{"title":"Antepartum Emergency Department Use and Associations with Maternal and Neonatal Outcomes in a Large Hospital System.","authors":"Thwisha Sabloak, Lynn M Yee, Joe Feinglass","doi":"10.1089/whr.2023.0072","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Prenatal care in the United States has remained unchanged for decades, with pregnant patients often experiencing high rates of hospital emergency department (ED) visits. It is unknown how many of these ED visits are potentially preventable with better access to timely and effective outpatient or home prenatal care. This multihospital health system quality improvement study was undertaken to analyze patient risk factors for acute antepartum hospital use as well as associations with adverse maternal and neonatal birth outcomes.</p><p><strong>Methods: </strong>The retrospective cohort study analyzed electronic health record and administrative data on ED visits in the 270 days before a delivery admission for alive, singleton births at nine system hospitals over 52 months. We use logistic regression to estimate the likelihood of hospital use by patient demographic and clinical characteristics and present the association of acute antepartum hospital use with maternal and neonatal birth outcomes.</p><p><strong>Results: </strong>Overall, 17.5% of 68,200 patients had antepartum ED visits, including 248 inpatient admissions, with significant variation between hospitals. As compared to non-Hispanic white patients, Hispanic and especially non-Hispanic Black and Medicaid patients had significantly higher odds of acute antepartum hospital use as did patients with preexisting conditions. Birth outcomes were significantly (<i>p</i> < 0.01) worse among individuals with antepartum hospital utilization.</p><p><strong>Conclusion: </strong>Acute antepartum hospital use was concentrated among lower income, minority patients, and those with chronic conditions with significant variation across system hospitals. There is a need for research into innovations in prenatal care that are best at reaching our most vulnerable patients, reducing preventable hospital utilization, and improving birth outcomes.</p>","PeriodicalId":75329,"journal":{"name":"Women's health reports (New Rochelle, N.Y.)","volume":"4 1","pages":"562-570"},"PeriodicalIF":1.8000,"publicationDate":"2023-12-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10719645/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Women's health reports (New Rochelle, N.Y.)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1089/whr.2023.0072","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Prenatal care in the United States has remained unchanged for decades, with pregnant patients often experiencing high rates of hospital emergency department (ED) visits. It is unknown how many of these ED visits are potentially preventable with better access to timely and effective outpatient or home prenatal care. This multihospital health system quality improvement study was undertaken to analyze patient risk factors for acute antepartum hospital use as well as associations with adverse maternal and neonatal birth outcomes.
Methods: The retrospective cohort study analyzed electronic health record and administrative data on ED visits in the 270 days before a delivery admission for alive, singleton births at nine system hospitals over 52 months. We use logistic regression to estimate the likelihood of hospital use by patient demographic and clinical characteristics and present the association of acute antepartum hospital use with maternal and neonatal birth outcomes.
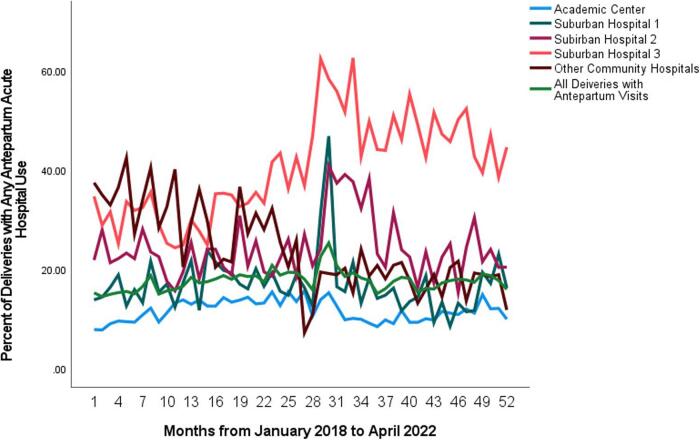
Results: Overall, 17.5% of 68,200 patients had antepartum ED visits, including 248 inpatient admissions, with significant variation between hospitals. As compared to non-Hispanic white patients, Hispanic and especially non-Hispanic Black and Medicaid patients had significantly higher odds of acute antepartum hospital use as did patients with preexisting conditions. Birth outcomes were significantly (p < 0.01) worse among individuals with antepartum hospital utilization.
Conclusion: Acute antepartum hospital use was concentrated among lower income, minority patients, and those with chronic conditions with significant variation across system hospitals. There is a need for research into innovations in prenatal care that are best at reaching our most vulnerable patients, reducing preventable hospital utilization, and improving birth outcomes.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
