Variation of Practice in Prophylactic Protocol to Reduce Prosthetic Joint Infection in Primary Hip and Knee Arthroplasty: A National Survey in the United Kingdom.
James Morris, Lee Hoggett, Sophie Rogers, John Ranson, Andrew Sloan
{"title":"Variation of Practice in Prophylactic Protocol to Reduce Prosthetic Joint Infection in Primary Hip and Knee Arthroplasty: A National Survey in the United Kingdom.","authors":"James Morris, Lee Hoggett, Sophie Rogers, John Ranson, Andrew Sloan","doi":"10.5371/hp.2023.35.4.228","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Prosthetic joint infection (PJI) has an enormous physiological and psychological burden on patients. Surgeons rightly wish to minimise this risk. It has been shown that a standardised, evidence-based approach to perioperative care leads to better patient outcomes. A review of current practice was conducted using a cross-sectional survey among surgeons at multiple centers nationwide.</p><p><strong>Materials and methods: </strong>An 11-question electronic survey was circulated to hip and knee arthroplasty consultants nationally via the BOA (British Orthopaedic Association) e-newsletter.</p><p><strong>Results: </strong>The respondents included 56 consultants working across 19 different trusts. Thirty-four (60.7%) screen patients for asymptomatic bacteriuria (ASB) preoperatively, with 19 (55.9%) would treating with antibiotics. Fifty-six (100%) screen for methicillin-resistant <i>Staphylococcus aureus</i> and treat if positive. Only 15 (26.8%) screen for methicillin-sensitive <i>S. aureus</i> (MSSA) or empirically eradicate. Zero (0%) routinely catheterise patients perioperatively. Forty-one (73.2%) would give intramuscular or intravenous gentamicin for a perioperative catheterisation. All surgeons use laminar flow theatres. Twenty-six (46.4%) use only an impervious gown, 6 (10.7%) exhaust pipes, and 24 (42.3%) surgical helmet system. Five different antimicrobial prophylaxis regimens are used 9 (16.1%) cefuroxime, 2 (3.6%) flucloxacillin, 19 (33.9%) flucloxacillin and gentamicin, 10 (17.9%) teicoplanin, 16 (28.6%) teicoplanin and gentamicin. Twenty-two (39.3%) routinely give further doses.</p><p><strong>Conclusion: </strong>ASB screening, treatment and intramuscular gentamicin for perioperative catheterisation is routinely practiced despite no supporting evidence base. MSSA screening and treatment is underutilised. Multiple antibiotic regimens exist despite little variation in organisms in PJI. Practice varies between surgeons and centers, we should all be practicing evidence-based medicine.</p>","PeriodicalId":73239,"journal":{"name":"Hip & pelvis","volume":"35 4","pages":"228-232"},"PeriodicalIF":0.0000,"publicationDate":"2023-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10728051/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hip & pelvis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5371/hp.2023.35.4.228","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/12/4 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Prosthetic joint infection (PJI) has an enormous physiological and psychological burden on patients. Surgeons rightly wish to minimise this risk. It has been shown that a standardised, evidence-based approach to perioperative care leads to better patient outcomes. A review of current practice was conducted using a cross-sectional survey among surgeons at multiple centers nationwide.
Materials and methods: An 11-question electronic survey was circulated to hip and knee arthroplasty consultants nationally via the BOA (British Orthopaedic Association) e-newsletter.
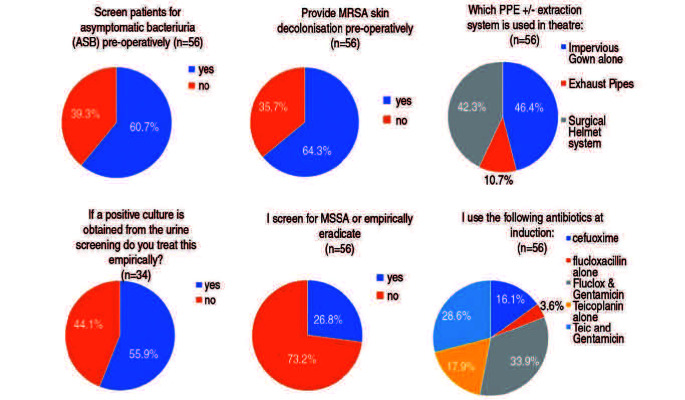
Results: The respondents included 56 consultants working across 19 different trusts. Thirty-four (60.7%) screen patients for asymptomatic bacteriuria (ASB) preoperatively, with 19 (55.9%) would treating with antibiotics. Fifty-six (100%) screen for methicillin-resistant Staphylococcus aureus and treat if positive. Only 15 (26.8%) screen for methicillin-sensitive S. aureus (MSSA) or empirically eradicate. Zero (0%) routinely catheterise patients perioperatively. Forty-one (73.2%) would give intramuscular or intravenous gentamicin for a perioperative catheterisation. All surgeons use laminar flow theatres. Twenty-six (46.4%) use only an impervious gown, 6 (10.7%) exhaust pipes, and 24 (42.3%) surgical helmet system. Five different antimicrobial prophylaxis regimens are used 9 (16.1%) cefuroxime, 2 (3.6%) flucloxacillin, 19 (33.9%) flucloxacillin and gentamicin, 10 (17.9%) teicoplanin, 16 (28.6%) teicoplanin and gentamicin. Twenty-two (39.3%) routinely give further doses.
Conclusion: ASB screening, treatment and intramuscular gentamicin for perioperative catheterisation is routinely practiced despite no supporting evidence base. MSSA screening and treatment is underutilised. Multiple antibiotic regimens exist despite little variation in organisms in PJI. Practice varies between surgeons and centers, we should all be practicing evidence-based medicine.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
