{"title":"Co-occurrence and inheritance of two typically sporadic neurogenetic disorders","authors":"Amanda Nagy, Hannah Brooks, Ann M. Neumeyer","doi":"10.1002/cns3.20053","DOIUrl":null,"url":null,"abstract":"<p>We describe a 13-year-old male diagnosed with two rare neurogenetic disorders, transducin (beta)-like X-linked receptor 1 (<i>TBL1XR1</i>)-related disorder and Bainbridge–Ropers syndrome (BRPS), caused by pathogenic variants in additional sex combs-like 3 (<i>ASXL3</i>). Each variant was inherited from an affected parent, although the parents each exhibited much milder phenotypes than the child. <i>TBL1XR1</i>, a widely expressed transcriptional regulator,<span><sup>1</sup></span> has been implicated in a range of neurodevelopmental disorders.<span><sup>2</sup></span> <i>TBL1XR1</i>-related disorder includes both Pierpont syndrome, a disorder associated with characteristic dysmorphism, including short stature, along with developmental delay, epilepsy, and feeding difficulties,<span><sup>3, 4</sup></span> and non-Pierpont presentations, including autism spectrum disorder (ASD), intellectual disability (ID), attention deficit hyperactivity disorder (ADHD), epilepsy, and schizophrenia.<span><sup>2</sup></span> Heterozygous pathogenic variants in the <i>ASXL3</i> transcriptional regulator cause BRPS, characterized by developmental delay with significant language impairment, ID, ASD, feeding difficulties, epilepsy, and dysmorphism.<span><sup>5</sup></span> Nonspecific clinical features that overlap with other genetic syndromes make <i>TBL1XR1</i>-related disorder and BRPS difficult to recognize and diagnose. Further, both disorders typically arise from de novo variants, with few cases of either disorder previously reported to be inherited.</p><p>The patient is a 13-year-old Hispanic male found to have a maternally inherited pathogenic <i>ASXL3</i> variant [c.4678C > T, p.(R1560*) in exon 12] and paternally inherited pathogenic <i>TBL1XR1</i> variant [c.1291C > T, p.(R431*) in exon 14]. Genetic testing was done by GeneDx using their autism/ID expanded panel with DNA analyzed via next-generation sequencing with copy-number variant calling. Both variants were classified as pathogenic by GeneDx using the 2015 guidelines published by the American College of Medical Genetics and Genomics and the Association for Molecular Pathology.<span><sup>6</sup></span></p><p>His mother has mild ID, ASD traits, ADHD, febrile seizures, and anxiety. His father has been diagnosed with Asperger syndrome, bipolar disorder, fetal alcohol syndrome, ID, ADHD, substance use disorder, anxiety, depression, and psychosis. There are no siblings. The patient was born full term at 6 pounds by Cesarean section due to maternal fever and an amniotic fluid leak. He spent one night in the neonatal intensive care unit for presumed infection. Perinatal difficulties included latching issues, tongue tie, extension contracture of the left hand that corrected over time, reflux, and poor/irritable sleep.</p><p>His initial development was normal; however, regression began after a fever at 18 months. Nearly all verbal and communication skills were lost. He made repetitive sounds, stopped playing with toys, and became less interested in people.</p><p>Neurological diagnoses include hypotonia, seizures at 6 weeks, and autism level 3 at 30 months. There is no known hearing deficit. Behaviorally, he has intermittent explosive disorder, stereotypic movement disorder with self-injurious behavior, generalized anxiety disorder, ADHD combined type, and insomnia. He had recurrent otitis and tonsillitis, a tonsillectomy, adenoidectomy, and frenulectomy. Magnetic resonance imaging findings at age 9 years revealed a cavernous malformation versus less likely a low-grade glioma. Electroencephalogram (EEG) at age 12 years recorded left, right, bilateral frontal, and frontal temporal spike-wave epileptiform potentials with increased activity during sleep. He was diagnosed with focal epilepsy with impaired consciousness based on EEG findings and reported episodes of staring and becoming stiff and unresponsive lasting less than a minute, followed by a period of fatigue, possibly triggered by aggressive behavior or emotion. No seizures were captured on EEG, however.</p><p>At 13 years, he is minimally verbal with a few two-word phrases. He walks, swims, bikes, and has social intent. He has ID, intact cranial nerves, and a symmetric motor exam. He has feeding difficulties, poor weight gain, and multiple sensory sensitivities. Some distinctive features often seen with BRPS and <i>TBL1XR1</i>-related disorder were present (Figure 1), while others such as fat pads on the hands and feet and hearing loss were absent. His mood is frequently irritable or anxious. At the time of his neurologic assessment at age 12 years, he was noted to have short stature (136.5 cm, 2 percentile) and corresponding low weight (24.9 kg, <1 percentile) but was normocephalic (53.5 cm, 37 percentile).</p><p>We describe a child with both <i>TBL1XR1</i>-related disorder and BRPS. He exhibits multiple phenotypic features common to each disorder, including ASD, developmental delay with severe language impairment, epilepsy, and feeding difficulties. The parents, although diagnosed with ASD, ID, and seizures, are more mildly affected. As both BRPS and <i>TBL1XR1</i>-related disorder have rarely been reported to be inherited, it is not clear whether the clinical differences are caused by the co-occurrence of two genetic disorders, particularly given that both are transcriptional regulators acting on nuclear receptors, or intrafamilial phenotypic variability in either disorder or both disorders. This child adds to the few reports documenting patients with inherited BRPS and <i>TBL1XR1</i>-related disorder.</p><p><b>Amanda Nagy</b>: Data curation; writing—original draft; writing—review and editing. <b>Hannah Brooks</b>: Data curation; writing—original draft. <b>Ann M. Neumeyer</b>: Data curation; supervision; writing—review and editing.</p><p>Ann M. Neumeyer is on the editorial board of <i>Annals of the Child Neurology Society</i>. The remaining authors declare no conflict of interest.</p>","PeriodicalId":72232,"journal":{"name":"Annals of the Child Neurology Society","volume":"2 1","pages":"79-81"},"PeriodicalIF":0.0000,"publicationDate":"2023-12-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cns3.20053","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of the Child Neurology Society","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cns3.20053","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
We describe a 13-year-old male diagnosed with two rare neurogenetic disorders, transducin (beta)-like X-linked receptor 1 (TBL1XR1)-related disorder and Bainbridge–Ropers syndrome (BRPS), caused by pathogenic variants in additional sex combs-like 3 (ASXL3). Each variant was inherited from an affected parent, although the parents each exhibited much milder phenotypes than the child. TBL1XR1, a widely expressed transcriptional regulator,1 has been implicated in a range of neurodevelopmental disorders.2TBL1XR1-related disorder includes both Pierpont syndrome, a disorder associated with characteristic dysmorphism, including short stature, along with developmental delay, epilepsy, and feeding difficulties,3, 4 and non-Pierpont presentations, including autism spectrum disorder (ASD), intellectual disability (ID), attention deficit hyperactivity disorder (ADHD), epilepsy, and schizophrenia.2 Heterozygous pathogenic variants in the ASXL3 transcriptional regulator cause BRPS, characterized by developmental delay with significant language impairment, ID, ASD, feeding difficulties, epilepsy, and dysmorphism.5 Nonspecific clinical features that overlap with other genetic syndromes make TBL1XR1-related disorder and BRPS difficult to recognize and diagnose. Further, both disorders typically arise from de novo variants, with few cases of either disorder previously reported to be inherited.
The patient is a 13-year-old Hispanic male found to have a maternally inherited pathogenic ASXL3 variant [c.4678C > T, p.(R1560*) in exon 12] and paternally inherited pathogenic TBL1XR1 variant [c.1291C > T, p.(R431*) in exon 14]. Genetic testing was done by GeneDx using their autism/ID expanded panel with DNA analyzed via next-generation sequencing with copy-number variant calling. Both variants were classified as pathogenic by GeneDx using the 2015 guidelines published by the American College of Medical Genetics and Genomics and the Association for Molecular Pathology.6
His mother has mild ID, ASD traits, ADHD, febrile seizures, and anxiety. His father has been diagnosed with Asperger syndrome, bipolar disorder, fetal alcohol syndrome, ID, ADHD, substance use disorder, anxiety, depression, and psychosis. There are no siblings. The patient was born full term at 6 pounds by Cesarean section due to maternal fever and an amniotic fluid leak. He spent one night in the neonatal intensive care unit for presumed infection. Perinatal difficulties included latching issues, tongue tie, extension contracture of the left hand that corrected over time, reflux, and poor/irritable sleep.
His initial development was normal; however, regression began after a fever at 18 months. Nearly all verbal and communication skills were lost. He made repetitive sounds, stopped playing with toys, and became less interested in people.
Neurological diagnoses include hypotonia, seizures at 6 weeks, and autism level 3 at 30 months. There is no known hearing deficit. Behaviorally, he has intermittent explosive disorder, stereotypic movement disorder with self-injurious behavior, generalized anxiety disorder, ADHD combined type, and insomnia. He had recurrent otitis and tonsillitis, a tonsillectomy, adenoidectomy, and frenulectomy. Magnetic resonance imaging findings at age 9 years revealed a cavernous malformation versus less likely a low-grade glioma. Electroencephalogram (EEG) at age 12 years recorded left, right, bilateral frontal, and frontal temporal spike-wave epileptiform potentials with increased activity during sleep. He was diagnosed with focal epilepsy with impaired consciousness based on EEG findings and reported episodes of staring and becoming stiff and unresponsive lasting less than a minute, followed by a period of fatigue, possibly triggered by aggressive behavior or emotion. No seizures were captured on EEG, however.
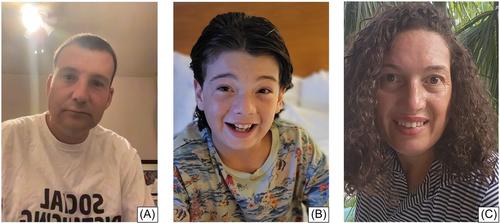
At 13 years, he is minimally verbal with a few two-word phrases. He walks, swims, bikes, and has social intent. He has ID, intact cranial nerves, and a symmetric motor exam. He has feeding difficulties, poor weight gain, and multiple sensory sensitivities. Some distinctive features often seen with BRPS and TBL1XR1-related disorder were present (Figure 1), while others such as fat pads on the hands and feet and hearing loss were absent. His mood is frequently irritable or anxious. At the time of his neurologic assessment at age 12 years, he was noted to have short stature (136.5 cm, 2 percentile) and corresponding low weight (24.9 kg, <1 percentile) but was normocephalic (53.5 cm, 37 percentile).
We describe a child with both TBL1XR1-related disorder and BRPS. He exhibits multiple phenotypic features common to each disorder, including ASD, developmental delay with severe language impairment, epilepsy, and feeding difficulties. The parents, although diagnosed with ASD, ID, and seizures, are more mildly affected. As both BRPS and TBL1XR1-related disorder have rarely been reported to be inherited, it is not clear whether the clinical differences are caused by the co-occurrence of two genetic disorders, particularly given that both are transcriptional regulators acting on nuclear receptors, or intrafamilial phenotypic variability in either disorder or both disorders. This child adds to the few reports documenting patients with inherited BRPS and TBL1XR1-related disorder.
Amanda Nagy: Data curation; writing—original draft; writing—review and editing. Hannah Brooks: Data curation; writing—original draft. Ann M. Neumeyer: Data curation; supervision; writing—review and editing.
Ann M. Neumeyer is on the editorial board of Annals of the Child Neurology Society. The remaining authors declare no conflict of interest.
由于BRPS和TBL1XR1相关障碍很少被报道为遗传性疾病,目前尚不清楚临床差异是由两种遗传性疾病同时存在造成的,特别是考虑到这两种疾病都是作用于核受体的转录调节剂,还是由其中一种疾病或两种疾病的家庭内部表型变异造成的。Amanda Nagy:数据整理;写作-原稿;写作-审阅和编辑。汉娜-布鲁克斯数据整理;写作-原稿。Ann M. Neumeyer:Ann M. Neumeyer是《儿童神经病学年报》(Annals of the Child Neurology Society)的编辑委员会成员。其余作者声明无利益冲突。


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
