Michele Vitacca, Mara Paneroni, Nicolino Ambrosino
{"title":"Rehabilitation complexity scale and reimbursement of in-hospital pulmonary rehabilitation.","authors":"Michele Vitacca, Mara Paneroni, Nicolino Ambrosino","doi":"10.4081/mrm.2023.936","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The use of case-based reimbursement for medical rehabilitation is greatly discussed. The investigators explored the relationship between disability and reimbursement opportunities in individuals with respiratory diseases undergoing in-hospital pulmonary rehabilitation (PR), considering the correlation (if any) between the Rehabilitation Complexity Scale (RCS-E v13) scores used at admission and the actual reimbursement.</p><p><strong>Methods: </strong>This study is part of a larger prospective multicenter study conducted by eight Pulmonary Rehabilitation Units in Italy. Here, investigators considered only data from the Lombardy Region. On January 30<sup>th</sup> or February 28<sup>th</sup>, 2023, participants were allocated according to the main DRG into 4 groups [tracheostomized/ventilated (TX/V), chronic respiratory failure (CRF), COPD, and miscellaneous group]. We recorded anthropometrics, diagnosis, international outcome measures, and calculated admission and discharge RCS-E v13 scores and hospital stay reimbursement according to the healthcare system (HS).</p><p><strong>Results: </strong>Three hundred and sixteen participants were evaluated. Patients were elderly, in the majority of cases with CRF, presenting comorbidities, disability, dyspnea, and reduced effort tolerance. At admission, RCS-E v13 showed an average moderate value of complexity. The median (IQR) HS reimbursement/stay was different among groups. RCSE v13 evaluated at admission was weakly (r=0.3471), but significantly related to the HS reimbursement/stay (p<0.0001) mainly due to TX/V and miscellaneous subgroups, while no relationship was found for COPD and CRF patients. After PR, all outcome measures improved significantly in all groups (p<0.001 for all). Higher RCS-E v13 scores at admission did not correspond to a proper amount of reimbursement, being this latter under- or over-estimated if compared to needs assessed by RCS-E v13. RCS-E v13 at discharge decreased for all subgroups (range from -6 to -11) reaching a low value of complexity.</p><p><strong>Conclusions: </strong>The RCS-E v13 disability score does not fully mirror the HS reimbursement for patients undergoing inhospital PR.</p>","PeriodicalId":51135,"journal":{"name":"Multidisciplinary Respiratory Medicine","volume":"18 1","pages":"936"},"PeriodicalIF":1.6000,"publicationDate":"2023-11-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10726991/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Multidisciplinary Respiratory Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4081/mrm.2023.936","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/17 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The use of case-based reimbursement for medical rehabilitation is greatly discussed. The investigators explored the relationship between disability and reimbursement opportunities in individuals with respiratory diseases undergoing in-hospital pulmonary rehabilitation (PR), considering the correlation (if any) between the Rehabilitation Complexity Scale (RCS-E v13) scores used at admission and the actual reimbursement.
Methods: This study is part of a larger prospective multicenter study conducted by eight Pulmonary Rehabilitation Units in Italy. Here, investigators considered only data from the Lombardy Region. On January 30th or February 28th, 2023, participants were allocated according to the main DRG into 4 groups [tracheostomized/ventilated (TX/V), chronic respiratory failure (CRF), COPD, and miscellaneous group]. We recorded anthropometrics, diagnosis, international outcome measures, and calculated admission and discharge RCS-E v13 scores and hospital stay reimbursement according to the healthcare system (HS).
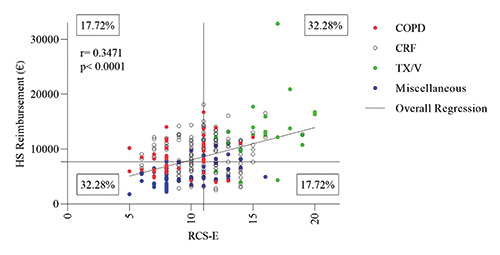
Results: Three hundred and sixteen participants were evaluated. Patients were elderly, in the majority of cases with CRF, presenting comorbidities, disability, dyspnea, and reduced effort tolerance. At admission, RCS-E v13 showed an average moderate value of complexity. The median (IQR) HS reimbursement/stay was different among groups. RCSE v13 evaluated at admission was weakly (r=0.3471), but significantly related to the HS reimbursement/stay (p<0.0001) mainly due to TX/V and miscellaneous subgroups, while no relationship was found for COPD and CRF patients. After PR, all outcome measures improved significantly in all groups (p<0.001 for all). Higher RCS-E v13 scores at admission did not correspond to a proper amount of reimbursement, being this latter under- or over-estimated if compared to needs assessed by RCS-E v13. RCS-E v13 at discharge decreased for all subgroups (range from -6 to -11) reaching a low value of complexity.
Conclusions: The RCS-E v13 disability score does not fully mirror the HS reimbursement for patients undergoing inhospital PR.
期刊介绍:
Multidisciplinary Respiratory Medicine is the official journal of the Italian Respiratory Society - Società Italiana di Pneumologia (IRS/SIP). The journal publishes on all aspects of respiratory medicine and related fields, with a particular focus on interdisciplinary and translational research.
The interdisciplinary nature of the journal provides a unique opportunity for researchers, clinicians and healthcare professionals across specialties to collaborate and exchange information. The journal provides a high visibility platform for the publication and dissemination of top quality original scientific articles, reviews and important position papers documenting clinical and experimental advances.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
