Frank Detterbeck , Sora Ely , Brooks Udelsman , Justin Blasberg , Daniel Boffa , Andrew Dhanasopon , Vincnet Mase , Gavitt Woodard
{"title":"So Now We Know—Reflections on the Extent of Resection for Stage I Lung Cancer","authors":"Frank Detterbeck , Sora Ely , Brooks Udelsman , Justin Blasberg , Daniel Boffa , Andrew Dhanasopon , Vincnet Mase , Gavitt Woodard","doi":"10.1016/j.cllc.2023.12.007","DOIUrl":null,"url":null,"abstract":"<div><p>Lobectomy has been the standard treatment for stage I lung cancer in healthy patients, largely based on a randomized trial published in 1995. Nevertheless, research has continued regarding the role of sublobar resection. Three additional randomized trials addressing resection extent in healthy patients have recently been published. These 4 trials involve differences in design, eligibility, interventions, and intraoperative processes. Patients were ineligible if intraoperative assessment demonstrated stage > IA or inadequate resection margins. All trials consistently show no differences in perioperative morbidity, mortality, and postoperative changes in lung function between sublobar resection and lobectomy—consistent with other nonrandomized evidence. Long-term outcomes are generally encouraging of lesser resection, but some inconsistencies are apparent. The 2 larger recent trials demonstrated no overall survival difference while the others suggested better survival after lobectomy versus sublobar resection. Recurrence-free survival was found to be the same after lobectomy versus sublobar resection in 3 trials, despite higher locoregional recurrences after sublobar resection. The low 5-year recurrence-free survival (64%, regardless of resection extent) in 1 recent trial highlights the need for further optimization. Thus, there is high-level evidence that sublobar resection is a reasonable alternative to lobectomy in healthy patients. However, variability in long-term results suggests that aspects of patients, tumors and interventions need to be better understood. Therefore, we propose to apply sublobar resection cautiously; especially because there are no short-term benefits. Sublobar resection requires careful attention to intraoperative details (nodes, margins), and may be best suited for less aggressive (eg, ground glass, slow growing) tumors.</p></div>","PeriodicalId":10490,"journal":{"name":"Clinical lung cancer","volume":"25 3","pages":"Pages e113-e123"},"PeriodicalIF":3.9000,"publicationDate":"2024-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical lung cancer","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1525730423002620","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/12/28 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
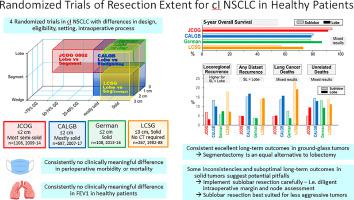
Lobectomy has been the standard treatment for stage I lung cancer in healthy patients, largely based on a randomized trial published in 1995. Nevertheless, research has continued regarding the role of sublobar resection. Three additional randomized trials addressing resection extent in healthy patients have recently been published. These 4 trials involve differences in design, eligibility, interventions, and intraoperative processes. Patients were ineligible if intraoperative assessment demonstrated stage > IA or inadequate resection margins. All trials consistently show no differences in perioperative morbidity, mortality, and postoperative changes in lung function between sublobar resection and lobectomy—consistent with other nonrandomized evidence. Long-term outcomes are generally encouraging of lesser resection, but some inconsistencies are apparent. The 2 larger recent trials demonstrated no overall survival difference while the others suggested better survival after lobectomy versus sublobar resection. Recurrence-free survival was found to be the same after lobectomy versus sublobar resection in 3 trials, despite higher locoregional recurrences after sublobar resection. The low 5-year recurrence-free survival (64%, regardless of resection extent) in 1 recent trial highlights the need for further optimization. Thus, there is high-level evidence that sublobar resection is a reasonable alternative to lobectomy in healthy patients. However, variability in long-term results suggests that aspects of patients, tumors and interventions need to be better understood. Therefore, we propose to apply sublobar resection cautiously; especially because there are no short-term benefits. Sublobar resection requires careful attention to intraoperative details (nodes, margins), and may be best suited for less aggressive (eg, ground glass, slow growing) tumors.
期刊介绍:
Clinical Lung Cancer is a peer-reviewed bimonthly journal that publishes original articles describing various aspects of clinical and translational research of lung cancer. Clinical Lung Cancer is devoted to articles on detection, diagnosis, prevention, and treatment of lung cancer. The main emphasis is on recent scientific developments in all areas related to lung cancer. Specific areas of interest include clinical research and mechanistic approaches; drug sensitivity and resistance; gene and antisense therapy; pathology, markers, and prognostic indicators; chemoprevention strategies; multimodality therapy; and integration of various approaches.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
