Jae Hoon Kim, Jae Kwang Yun, Chan Wook Kim, Hyeong Ryul Kim, Yong-Hee Kim
{"title":"Long-Term Outcomes of Colon Conduits in Surgery for Primary Esophageal Cancer: A Propensity Score-Matched Comparison to Gastric Conduits.","authors":"Jae Hoon Kim, Jae Kwang Yun, Chan Wook Kim, Hyeong Ryul Kim, Yong-Hee Kim","doi":"10.5090/jcs.23.074","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In the treatment of esophageal cancer, a gastric conduit is typically the first choice. However, when the stomach is not a viable option, the usual alternative is a colon conduit. This study compared the long-term surgical outcomes of gastric and colon conduits over the same interval and aimed to identify factors influencing the prognosis.</p><p><strong>Methods: </strong>A retrospective review was conducted of patients who underwent esophagectomy followed by reconstruction for primary esophageal cancer between January 2006 and December 2020.</p><p><strong>Results: </strong>The study included 1,545 patients, with a gastric conduit used for 1,429 (92.5%) and a colon conduit for 116 (7.5%). Using propensity-matched analysis, 116 patients were selected from each group for comparison. No significant difference was observed in long-term survival between the gastric and colon conduit groups, irrespective of anastomosis level and pathological stage. A higher proportion of patients in the colon conduit group experienced postoperative complications compared to the gastric conduit group (57.8% vs. 25%, p<0.001). Multivariable analysis revealed that age over 65 years, body mass index below 22.0 kg/m<sup>2</sup>, neoadjuvant therapy, postoperative anastomotic leakage, and renal failure were risk factors for overall survival in patients with a colon conduit. Regarding conduit-related complications, cervical anastomosis was the only significant risk factor among those with a colon conduit.</p><p><strong>Conclusion: </strong>Despite the association of colon conduits with high morbidity rates relative to gastric conduits, the long-term outcomes of colon conduits were acceptable. More consideration should be given perioperatively to the use of a colon conduit, particularly in cases involving cervical anastomosis.</p>","PeriodicalId":34499,"journal":{"name":"Journal of Chest Surgery","volume":"57 1","pages":"53-61"},"PeriodicalIF":1.0000,"publicationDate":"2024-01-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10792377/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Chest Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5090/jcs.23.074","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: In the treatment of esophageal cancer, a gastric conduit is typically the first choice. However, when the stomach is not a viable option, the usual alternative is a colon conduit. This study compared the long-term surgical outcomes of gastric and colon conduits over the same interval and aimed to identify factors influencing the prognosis.
Methods: A retrospective review was conducted of patients who underwent esophagectomy followed by reconstruction for primary esophageal cancer between January 2006 and December 2020.
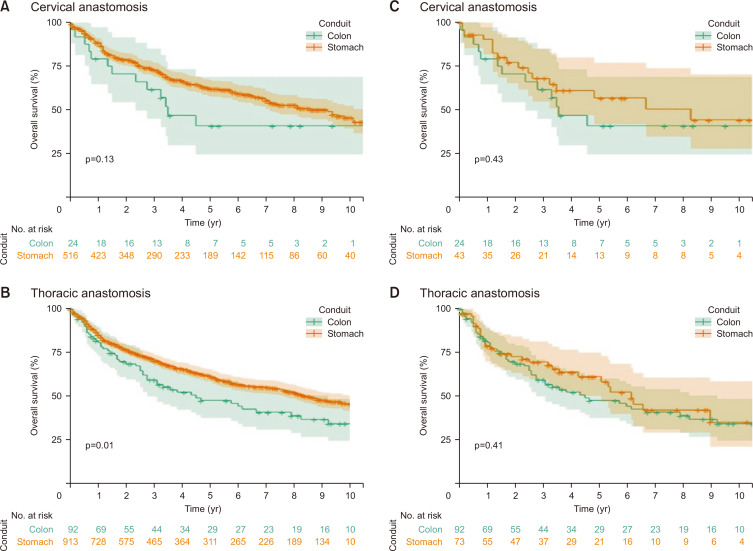
Results: The study included 1,545 patients, with a gastric conduit used for 1,429 (92.5%) and a colon conduit for 116 (7.5%). Using propensity-matched analysis, 116 patients were selected from each group for comparison. No significant difference was observed in long-term survival between the gastric and colon conduit groups, irrespective of anastomosis level and pathological stage. A higher proportion of patients in the colon conduit group experienced postoperative complications compared to the gastric conduit group (57.8% vs. 25%, p<0.001). Multivariable analysis revealed that age over 65 years, body mass index below 22.0 kg/m2, neoadjuvant therapy, postoperative anastomotic leakage, and renal failure were risk factors for overall survival in patients with a colon conduit. Regarding conduit-related complications, cervical anastomosis was the only significant risk factor among those with a colon conduit.
Conclusion: Despite the association of colon conduits with high morbidity rates relative to gastric conduits, the long-term outcomes of colon conduits were acceptable. More consideration should be given perioperatively to the use of a colon conduit, particularly in cases involving cervical anastomosis.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
