{"title":"Corticothalamic Responsive Neurostimulation for Focal Epilepsy: A Single-Center Experience.","authors":"David Burdette, Sanjay Patra, Lise Johnson","doi":"10.1097/WNP.0000000000001060","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Owing to its extensive, reciprocal connectivity with the cortex and other subcortical structures, the thalamus is considered an important target for neuromodulation in drug-resistant focal epilepsy. Using corticothalamic stimulation, it is possible to modulate both the thalamus and the cortical seizure onset zone. Limited published clinical experience describes corticothalamic stimulation with depth leads targeting one of the anterior (ANT), centromedian (centromedian nucleus), or pulvinar (PUL) thalamic nuclei. However, it is not clear which of these nuclei is the \"best\" therapeutic target.</p><p><strong>Methods: </strong>This study comprised a single-center experience with corticothalamic responsive neurostimulation using the RNS System to target these three thalamic nuclei. Presented here are the methods for target selection and device programming as well as clinical outcomes and a comparison of ictal and nonictal electrophysiological features.</p><p><strong>Results: </strong>In this small retrospective study ( N = 19), responsive corticothalamic neurostimulation was an effective therapy for 79% of patients (≥50% reduction in disabling seizure frequency), regardless of whether the thalamic lead was implanted in the ANT ( N = 2), PUL ( N = 6), or centromedian nucleus ( N = 11). Twenty-six percent of patients reported a reduction in disabling seizure frequency ≥90%. Both high frequency (≥100 Hz) and low (≤20 Hz) frequency were used to stimulate the thalamus depending on the patient's response and ability to tolerate higher charge densities. In all patients, a longer burst duration (2000-5000 ms) was ultimately implemented on the thalamic leads. Across patients, peaks in the intracranial EEG were observed at theta, beta, gamma, and sleep spindle frequencies. Changes in frequency content and distribution were observed over time in all three nuclei.</p><p><strong>Conclusions: </strong>These results indicate that both high frequency and low frequency corticothalamic responsive neurostimulation can potentially be an effective adjunctive therapy in drug-resistant focal epilepsy. These data can also contribute to a broader understanding of thalamic electrophysiology in the context of focal epilepsy.</p>","PeriodicalId":15516,"journal":{"name":"Journal of Clinical Neurophysiology","volume":" ","pages":"630-639"},"PeriodicalIF":1.7000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11520339/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Neurophysiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/WNP.0000000000001060","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/9 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Owing to its extensive, reciprocal connectivity with the cortex and other subcortical structures, the thalamus is considered an important target for neuromodulation in drug-resistant focal epilepsy. Using corticothalamic stimulation, it is possible to modulate both the thalamus and the cortical seizure onset zone. Limited published clinical experience describes corticothalamic stimulation with depth leads targeting one of the anterior (ANT), centromedian (centromedian nucleus), or pulvinar (PUL) thalamic nuclei. However, it is not clear which of these nuclei is the "best" therapeutic target.
Methods: This study comprised a single-center experience with corticothalamic responsive neurostimulation using the RNS System to target these three thalamic nuclei. Presented here are the methods for target selection and device programming as well as clinical outcomes and a comparison of ictal and nonictal electrophysiological features.
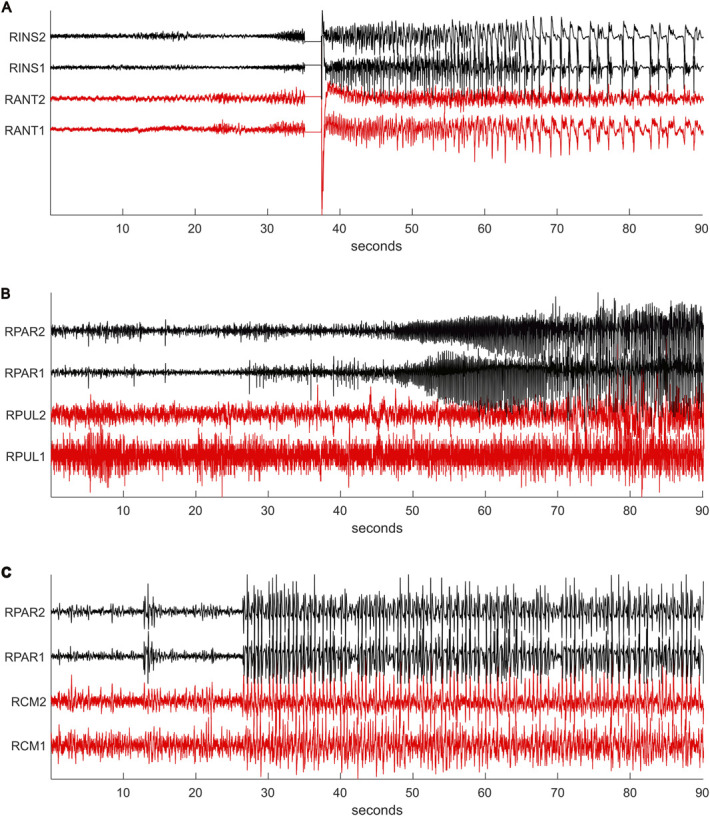
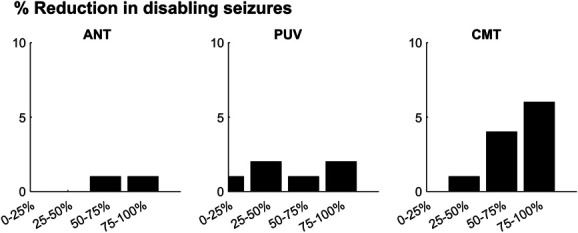
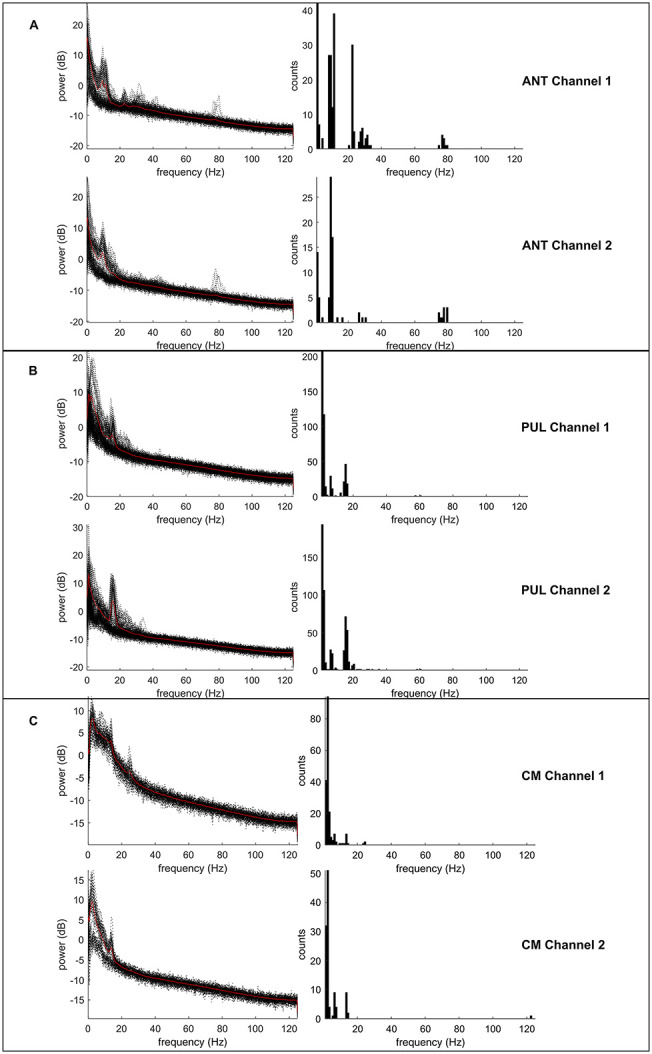
Results: In this small retrospective study ( N = 19), responsive corticothalamic neurostimulation was an effective therapy for 79% of patients (≥50% reduction in disabling seizure frequency), regardless of whether the thalamic lead was implanted in the ANT ( N = 2), PUL ( N = 6), or centromedian nucleus ( N = 11). Twenty-six percent of patients reported a reduction in disabling seizure frequency ≥90%. Both high frequency (≥100 Hz) and low (≤20 Hz) frequency were used to stimulate the thalamus depending on the patient's response and ability to tolerate higher charge densities. In all patients, a longer burst duration (2000-5000 ms) was ultimately implemented on the thalamic leads. Across patients, peaks in the intracranial EEG were observed at theta, beta, gamma, and sleep spindle frequencies. Changes in frequency content and distribution were observed over time in all three nuclei.
Conclusions: These results indicate that both high frequency and low frequency corticothalamic responsive neurostimulation can potentially be an effective adjunctive therapy in drug-resistant focal epilepsy. These data can also contribute to a broader understanding of thalamic electrophysiology in the context of focal epilepsy.
期刊介绍:
The Journal of Clinical Neurophysiology features both topical reviews and original research in both central and peripheral neurophysiology, as related to patient evaluation and treatment.
Official Journal of the American Clinical Neurophysiology Society.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
