{"title":"One-stage jaw reconstruction and prosthetic rehabilitation with an iliac flap: a case report and literature review.","authors":"Yi-Fan Kang, Yan-Jun Ge, Xiao-Ming Lv, Meng-Kun Ding, Xiao-Feng Shan, Zhi-Gang Cai","doi":"10.1186/s40902-024-00413-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>One-stage jaw reconstruction with fibular flap and prosthetic rehabilitation restores bony and dental continuity simultaneously. It was also called as \"jaw-in-a-day (JIAD)\" technique. However, bone volume and height of fibular flap may be insufficient for dental implant insertion. The provision of a considerable amount of bone makes an iliac flap the ideal choice in these cases. We present the first case report to document the use of one-stage jaw reconstruction and prosthetic rehabilitation with the iliac flap.</p><p><strong>Case presentation: </strong>We modified the conventional JIAD workflow to make it suitable for iliac flap. Two cases were presented who both underwent segmental mandibulectomy for ameloblastoma. Virtual surgical planning was performed in all cases. The iliac crest was positioned upward to provide cortical bone for achieving primary stability of dental implants. Similar to the \"all-on-4\" procedure, the iliac bone was placed 12 to 15 mm below the occlusal plane to create adequate space for the implant-retained prosthesis. Immediate implant-based dental rehabilitation was performed at same stage. The surgery was successful in all cases without any short-term complications. In the first postoperative week, patients were given a liquid diet through a nasal feeding tube. The liquid diet is advised until 1 month after the surgery. Thereafter, a soft diet is recommended. Patients were advised to resume routine mastication and normal diet 3 months after the surgery. Peri-implantitis occurred in one patient, and additional gingival graft was required. Postoperative function and esthetics were satisfactory at the last follow-up visit.</p><p><strong>Conclusions: </strong>One-stage jaw reconstruction and prosthetic rehabilitation with the iliac flap are safe and useful for restoring postoperative function and esthetics. It should be used in more cases with a longer follow-up in further studies.</p>","PeriodicalId":18357,"journal":{"name":"Maxillofacial Plastic and Reconstructive Surgery","volume":"46 1","pages":"3"},"PeriodicalIF":2.8000,"publicationDate":"2024-01-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10794675/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Maxillofacial Plastic and Reconstructive Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40902-024-00413-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"DENTISTRY, ORAL SURGERY & MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: One-stage jaw reconstruction with fibular flap and prosthetic rehabilitation restores bony and dental continuity simultaneously. It was also called as "jaw-in-a-day (JIAD)" technique. However, bone volume and height of fibular flap may be insufficient for dental implant insertion. The provision of a considerable amount of bone makes an iliac flap the ideal choice in these cases. We present the first case report to document the use of one-stage jaw reconstruction and prosthetic rehabilitation with the iliac flap.
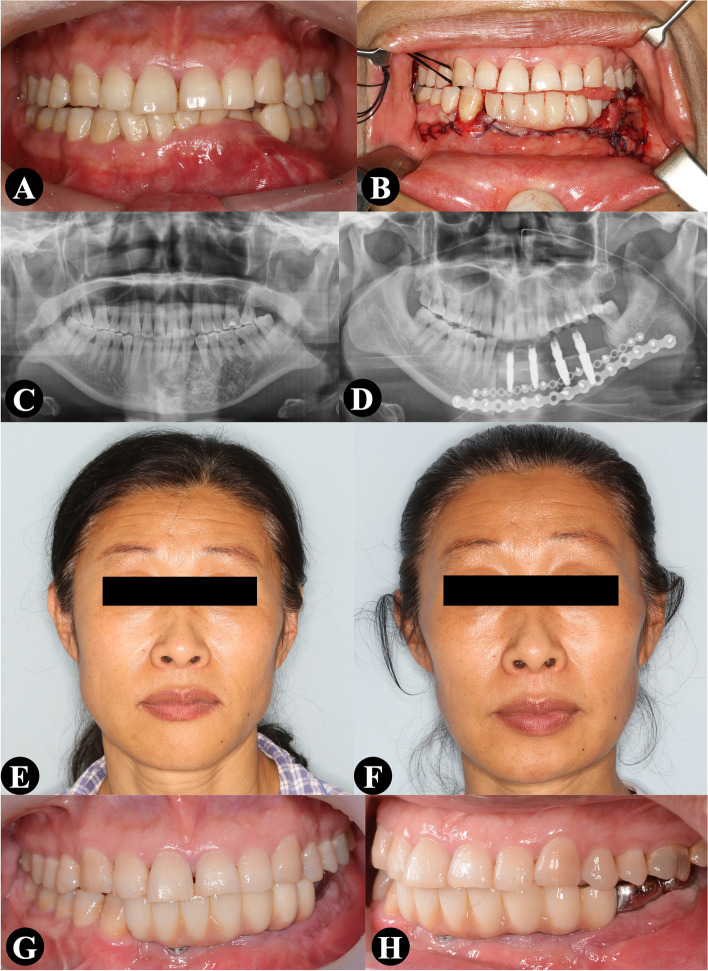
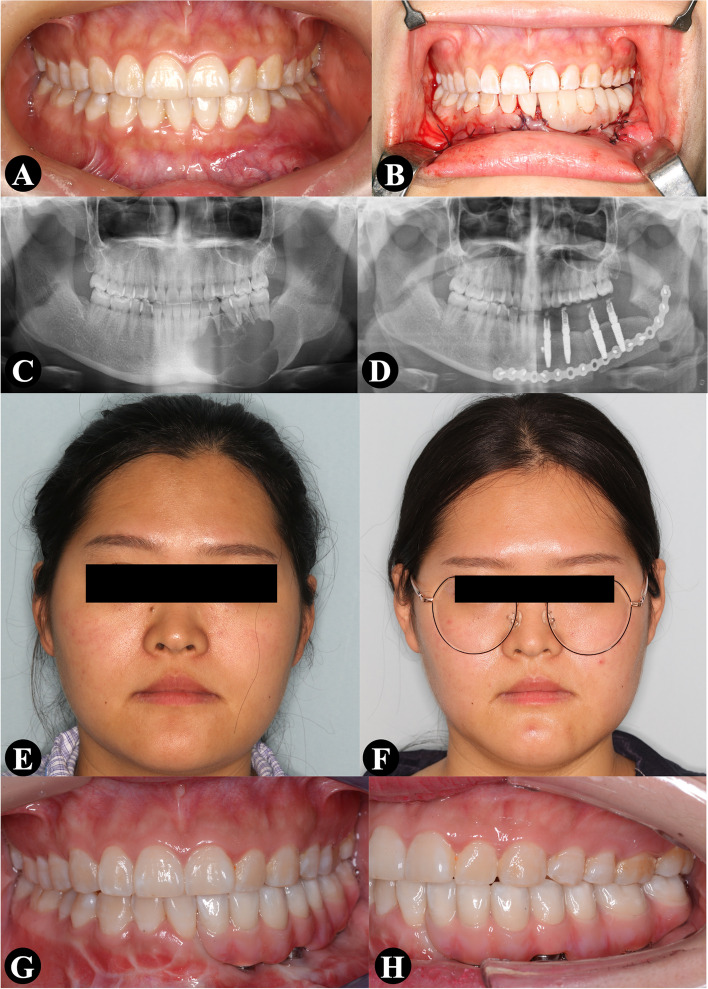
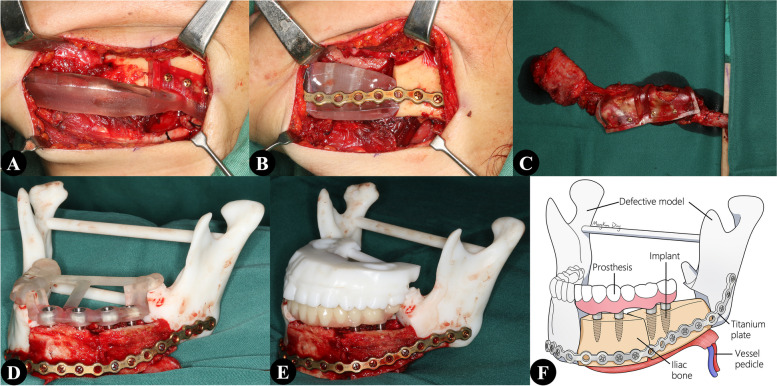
Case presentation: We modified the conventional JIAD workflow to make it suitable for iliac flap. Two cases were presented who both underwent segmental mandibulectomy for ameloblastoma. Virtual surgical planning was performed in all cases. The iliac crest was positioned upward to provide cortical bone for achieving primary stability of dental implants. Similar to the "all-on-4" procedure, the iliac bone was placed 12 to 15 mm below the occlusal plane to create adequate space for the implant-retained prosthesis. Immediate implant-based dental rehabilitation was performed at same stage. The surgery was successful in all cases without any short-term complications. In the first postoperative week, patients were given a liquid diet through a nasal feeding tube. The liquid diet is advised until 1 month after the surgery. Thereafter, a soft diet is recommended. Patients were advised to resume routine mastication and normal diet 3 months after the surgery. Peri-implantitis occurred in one patient, and additional gingival graft was required. Postoperative function and esthetics were satisfactory at the last follow-up visit.
Conclusions: One-stage jaw reconstruction and prosthetic rehabilitation with the iliac flap are safe and useful for restoring postoperative function and esthetics. It should be used in more cases with a longer follow-up in further studies.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
