{"title":"Familial Psychomotor Delay of an Uncommon Cause: Type II Congenital Methemoglobinemia.","authors":"Hager Barakizou, Selma Chaieb","doi":"10.1177/11795565241229007","DOIUrl":null,"url":null,"abstract":"<p><p>Methemoglobinemia is due to oxidization of divalent ferro-iron of hemoglobin to ferri-iron of methemoglobin (MetHb) which is incapable of transferring oxygen to tissues. This disease may be acquired by intoxication with oxidizing agents or inherited with a mutation of CYB5R3, the gene coding for the methemoglobin reductase or cytochrome B5 reductase 3 responsible for the reduction of MetHb to hemoglobin. We report the case of 2 sisters aged respectively of 15 and 8 months. They were born to a second-degree consanguineous marriage with a history of precocious and unexplained deaths in 3 relatives. Both sisters presented neurological features including psychomotor retardation, microcephaly, and axial hypotonia. Cerebral magnetic resonance imaging revealed cerebral atrophy in both cases associated with hypoplasia of the corpus callosum in the younger child. The association of neurological disability, cyanosis, and hypoxemia prompted a search for methemoglobinemia, with MetHB levels respectively of 26% and 15.8%in the 2 sisters. Initial treatment was based on methylene blue, then ascorbic acid. The genetic study revealed a c.463+8G>C mutation of CYB5R3 confirming the diagnosis of methemoglobinemia type II. The diagnosis of methemoglobinemia, although rare, should be considered in the presence of psychomotor retardation with cyanosis and subacute onset hypoxemia, especially in the presence of a family history.</p>","PeriodicalId":45027,"journal":{"name":"Clinical Medicine Insights-Pediatrics","volume":"18 ","pages":"11795565241229007"},"PeriodicalIF":1.2000,"publicationDate":"2024-01-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10832405/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights-Pediatrics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11795565241229007","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
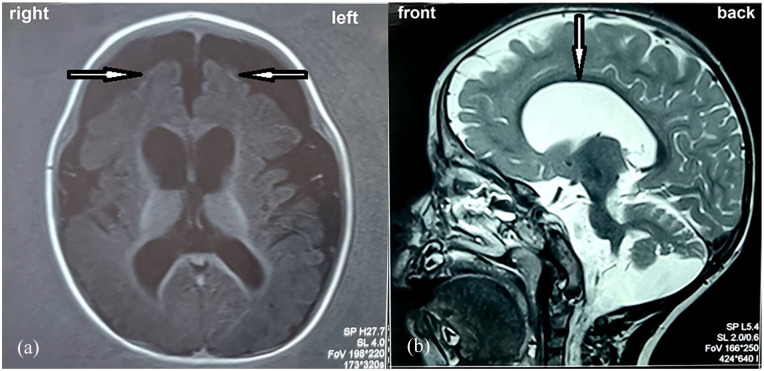
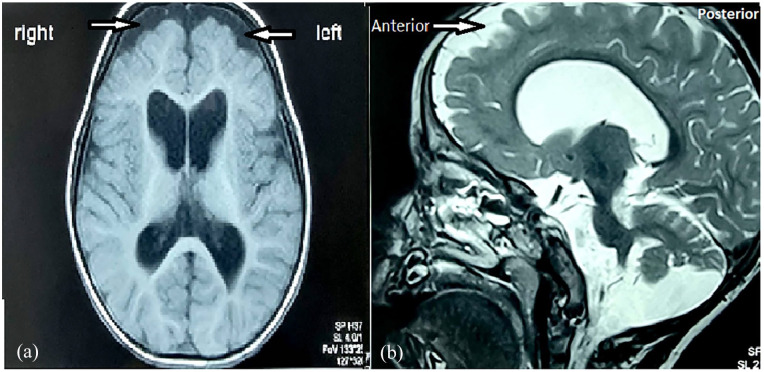
Methemoglobinemia is due to oxidization of divalent ferro-iron of hemoglobin to ferri-iron of methemoglobin (MetHb) which is incapable of transferring oxygen to tissues. This disease may be acquired by intoxication with oxidizing agents or inherited with a mutation of CYB5R3, the gene coding for the methemoglobin reductase or cytochrome B5 reductase 3 responsible for the reduction of MetHb to hemoglobin. We report the case of 2 sisters aged respectively of 15 and 8 months. They were born to a second-degree consanguineous marriage with a history of precocious and unexplained deaths in 3 relatives. Both sisters presented neurological features including psychomotor retardation, microcephaly, and axial hypotonia. Cerebral magnetic resonance imaging revealed cerebral atrophy in both cases associated with hypoplasia of the corpus callosum in the younger child. The association of neurological disability, cyanosis, and hypoxemia prompted a search for methemoglobinemia, with MetHB levels respectively of 26% and 15.8%in the 2 sisters. Initial treatment was based on methylene blue, then ascorbic acid. The genetic study revealed a c.463+8G>C mutation of CYB5R3 confirming the diagnosis of methemoglobinemia type II. The diagnosis of methemoglobinemia, although rare, should be considered in the presence of psychomotor retardation with cyanosis and subacute onset hypoxemia, especially in the presence of a family history.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
