Short-term mild hyperventilation on intracranial pressure, cerebral autoregulation, and oxygenation in acute brain injury patients: a prospective observational study.
Danilo Cardim, Alberto Giardina, Pietro Ciliberti, Denise Battaglini, Andrea Berardino, Antonio Uccelli, Marek Czosnyka, Luca Roccatagliata, Basil Matta, Nicolo Patroniti, Patricia R M Rocco, Chiara Robba
{"title":"Short-term mild hyperventilation on intracranial pressure, cerebral autoregulation, and oxygenation in acute brain injury patients: a prospective observational study.","authors":"Danilo Cardim, Alberto Giardina, Pietro Ciliberti, Denise Battaglini, Andrea Berardino, Antonio Uccelli, Marek Czosnyka, Luca Roccatagliata, Basil Matta, Nicolo Patroniti, Patricia R M Rocco, Chiara Robba","doi":"10.1007/s10877-023-01121-2","DOIUrl":null,"url":null,"abstract":"<p><p>Current guidelines suggest a target of partial pressure of carbon dioxide (PaCO<sub>2</sub>) of 32-35 mmHg (mild hypocapnia) as tier 2 for the management of intracranial hypertension. However, the effects of mild hyperventilation on cerebrovascular dynamics are not completely elucidated. The aim of this study is to evaluate the changes of intracranial pressure (ICP), cerebral autoregulation (measured through pressure reactivity index, PRx), and regional cerebral oxygenation (rSO<sub>2</sub>) parameters before and after induction of mild hyperventilation. Single center, observational study including patients with acute brain injury (ABI) admitted to the intensive care unit undergoing multimodal neuromonitoring and requiring titration of PaCO<sub>2</sub> values to mild hypocapnia as tier 2 for the management of intracranial hypertension. Twenty-five patients were included in this study (40% female), median age 64.7 years (Interquartile Range, IQR = 45.9-73.2). Median Glasgow Coma Scale was 6 (IQR = 3-11). After mild hyperventilation, PaCO<sub>2</sub> values decreased (from 42 (39-44) to 34 (32-34) mmHg, p < 0.0001), ICP and PRx significantly decreased (from 25.4 (24.1-26.4) to 17.5 (16-21.2) mmHg, p < 0.0001, and from 0.32 (0.1-0.52) to 0.12 (-0.03-0.23), p < 0.0001). rSO<sub>2</sub> was statistically but not clinically significantly reduced (from 60% (56-64) to 59% (54-61), p < 0.0001), but the arterial component of rSO<sub>2</sub> (ΔO<sub>2</sub>Hbi, changes in concentration of oxygenated hemoglobin of the total rSO<sub>2</sub>) decreased from 3.83 (3-6.2) μM.cm to 1.6 (0.5-3.1) μM.cm, p = 0.0001. Mild hyperventilation can reduce ICP and improve cerebral autoregulation, with minimal clinical effects on cerebral oxygenation. However, the arterial component of rSO<sub>2</sub> was importantly reduced. Multimodal neuromonitoring is essential when titrating PaCO<sub>2</sub> values for ICP management.</p>","PeriodicalId":15513,"journal":{"name":"Journal of Clinical Monitoring and Computing","volume":" ","pages":"753-762"},"PeriodicalIF":2.2000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11297838/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Monitoring and Computing","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10877-023-01121-2","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/4 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
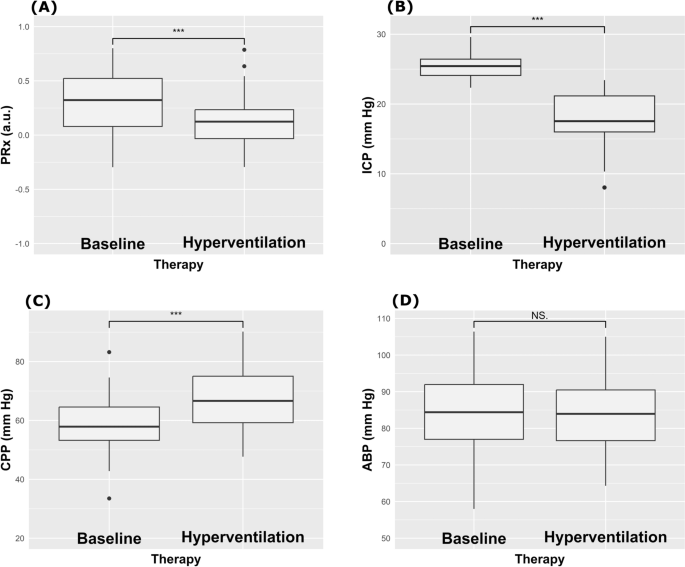
Current guidelines suggest a target of partial pressure of carbon dioxide (PaCO2) of 32-35 mmHg (mild hypocapnia) as tier 2 for the management of intracranial hypertension. However, the effects of mild hyperventilation on cerebrovascular dynamics are not completely elucidated. The aim of this study is to evaluate the changes of intracranial pressure (ICP), cerebral autoregulation (measured through pressure reactivity index, PRx), and regional cerebral oxygenation (rSO2) parameters before and after induction of mild hyperventilation. Single center, observational study including patients with acute brain injury (ABI) admitted to the intensive care unit undergoing multimodal neuromonitoring and requiring titration of PaCO2 values to mild hypocapnia as tier 2 for the management of intracranial hypertension. Twenty-five patients were included in this study (40% female), median age 64.7 years (Interquartile Range, IQR = 45.9-73.2). Median Glasgow Coma Scale was 6 (IQR = 3-11). After mild hyperventilation, PaCO2 values decreased (from 42 (39-44) to 34 (32-34) mmHg, p < 0.0001), ICP and PRx significantly decreased (from 25.4 (24.1-26.4) to 17.5 (16-21.2) mmHg, p < 0.0001, and from 0.32 (0.1-0.52) to 0.12 (-0.03-0.23), p < 0.0001). rSO2 was statistically but not clinically significantly reduced (from 60% (56-64) to 59% (54-61), p < 0.0001), but the arterial component of rSO2 (ΔO2Hbi, changes in concentration of oxygenated hemoglobin of the total rSO2) decreased from 3.83 (3-6.2) μM.cm to 1.6 (0.5-3.1) μM.cm, p = 0.0001. Mild hyperventilation can reduce ICP and improve cerebral autoregulation, with minimal clinical effects on cerebral oxygenation. However, the arterial component of rSO2 was importantly reduced. Multimodal neuromonitoring is essential when titrating PaCO2 values for ICP management.
期刊介绍:
The Journal of Clinical Monitoring and Computing is a clinical journal publishing papers related to technology in the fields of anaesthesia, intensive care medicine, emergency medicine, and peri-operative medicine.
The journal has links with numerous specialist societies, including editorial board representatives from the European Society for Computing and Technology in Anaesthesia and Intensive Care (ESCTAIC), the Society for Technology in Anesthesia (STA), the Society for Complex Acute Illness (SCAI) and the NAVAt (NAVigating towards your Anaestheisa Targets) group.
The journal publishes original papers, narrative and systematic reviews, technological notes, letters to the editor, editorial or commentary papers, and policy statements or guidelines from national or international societies. The journal encourages debate on published papers and technology, including letters commenting on previous publications or technological concerns. The journal occasionally publishes special issues with technological or clinical themes, or reports and abstracts from scientificmeetings. Special issues proposals should be sent to the Editor-in-Chief. Specific details of types of papers, and the clinical and technological content of papers considered within scope can be found in instructions for authors.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
