Adrian Peacock, Frances C Dehle, Oscar A Mesa Zapata, Francesca Gennari, Maro R I Williams, Nada Hamad, Stephen Larsen, Simon J Harrison, Colman Taylor
{"title":"Cost-Effectiveness of Extracorporeal Photopheresis in Patients With Chronic Graft-vs-Host Disease.","authors":"Adrian Peacock, Frances C Dehle, Oscar A Mesa Zapata, Francesca Gennari, Maro R I Williams, Nada Hamad, Stephen Larsen, Simon J Harrison, Colman Taylor","doi":"10.36469/001c.92028","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> The mainstay first-line therapy for chronic graft-vs-host disease (cGVHD) is corticosteroids; however, for steroid-refractory patients, there is a distinct lack of cost-effective or efficacious treatment. The aim of this study was to assess the cost-effectiveness of extracorporeal photopheresis (ECP) compared with standard-of-care therapies for the treatment of cGVHD in Australia. The study formed part of an application to the Australian Government to reimburse ECP for these patients. <b>Methods:</b> A cost-utility analysis was conducted comparing ECP to standard of care, which modeled the response to treatment and disease progression of cGVHD patients in Australia. Mycophenolate, tacrolimus, and cyclosporin comprised second-line standard of care based on a survey of Australian clinicians. Health states in the model included treatment response, disease progression, and death. Transition probabilities were obtained from Australian-specific registry data and randomized controlled evidence. Quality-of-life values were applied based on treatment response. The analysis considered costs of second-line treatment and disease management including immunosuppressants, hospitalizations and subsequent therapy. Disease-specific mortality was calculated for treatment response and progression. <b>Results:</b> Over a 10-year time horizon, ECP resulted in an average cost reduction of $23 999 and an incremental improvement of 1.10 quality-adjusted life-years per patient compared with standard of care. The sensitivity analysis demonstrated robustness over a range of plausible scenarios. <b>Conclusion:</b> This analysis demonstrates that ECP improves quality of life, minimizes the harms associated with immunosuppressant therapy, and is a highly cost-effective option for steroid-refractory cGVHD patients in Australia. Based in part on this analysis, ECP was listed on the Medicare Benefits Schedule for public reimbursement.</p>","PeriodicalId":16012,"journal":{"name":"Journal of Health Economics and Outcomes Research","volume":"11 1","pages":"23-31"},"PeriodicalIF":2.3000,"publicationDate":"2024-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10838062/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Health Economics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36469/001c.92028","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
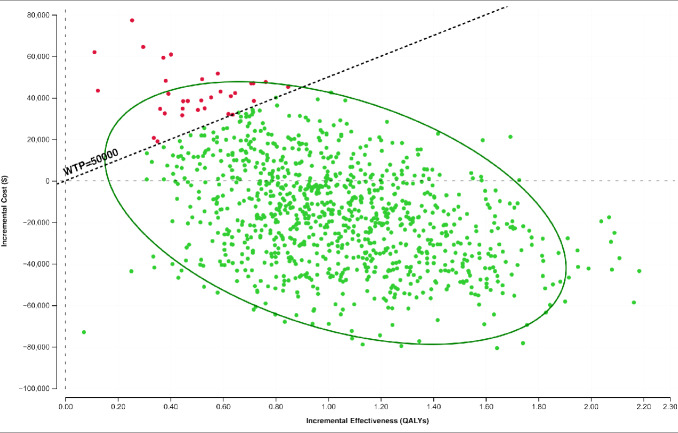
Background: The mainstay first-line therapy for chronic graft-vs-host disease (cGVHD) is corticosteroids; however, for steroid-refractory patients, there is a distinct lack of cost-effective or efficacious treatment. The aim of this study was to assess the cost-effectiveness of extracorporeal photopheresis (ECP) compared with standard-of-care therapies for the treatment of cGVHD in Australia. The study formed part of an application to the Australian Government to reimburse ECP for these patients. Methods: A cost-utility analysis was conducted comparing ECP to standard of care, which modeled the response to treatment and disease progression of cGVHD patients in Australia. Mycophenolate, tacrolimus, and cyclosporin comprised second-line standard of care based on a survey of Australian clinicians. Health states in the model included treatment response, disease progression, and death. Transition probabilities were obtained from Australian-specific registry data and randomized controlled evidence. Quality-of-life values were applied based on treatment response. The analysis considered costs of second-line treatment and disease management including immunosuppressants, hospitalizations and subsequent therapy. Disease-specific mortality was calculated for treatment response and progression. Results: Over a 10-year time horizon, ECP resulted in an average cost reduction of $23 999 and an incremental improvement of 1.10 quality-adjusted life-years per patient compared with standard of care. The sensitivity analysis demonstrated robustness over a range of plausible scenarios. Conclusion: This analysis demonstrates that ECP improves quality of life, minimizes the harms associated with immunosuppressant therapy, and is a highly cost-effective option for steroid-refractory cGVHD patients in Australia. Based in part on this analysis, ECP was listed on the Medicare Benefits Schedule for public reimbursement.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
