Charlotte Reich, Elena Weigl, Anne-Sophie Holler, William Lee, Michael Harrison, Oliver J Muensterer
{"title":"Repair of complex esophageal atresia with tracheobronchial remnant using special magnets.","authors":"Charlotte Reich, Elena Weigl, Anne-Sophie Holler, William Lee, Michael Harrison, Oliver J Muensterer","doi":"10.1055/s-0044-1779042","DOIUrl":null,"url":null,"abstract":"<p><p>Esophageal atresia (EA) repair can be complicated by associated malformations such as a tracheobronchial remnant in the distal esophagus. We describe our experience with a patient found to have long-gap EA with a distal cartilaginous ring who was managed using a combination of esophageal lengthening and magnetic compression anastomosis. A 5-month-old girl was referred to us from an outside hospital with type C EA including a very high upper pouch. She had undergone a prior thoracotomy with fistula ligation during which a clip was placed on the lower esophagus, leaving a 2-cm diverticulum on the trachea and a short lower esophageal pouch. Upon endoscopic evaluation at our center, we found a tracheobronchial remnant in the lower esophagus between the clip and the carina. An open thoracotomy was performed to approximate the esophageal pouches and a magnet anchor (Connect EA, Myka Laboratories, San Francisco, California, United States) was placed retrograde through the distal esophageal cartilaginous ring into the lower pouch. On postoperative day 8, after adequate growth and decreased pouch tension, a second magnetic anchor was placed endoscopically to the upper pouch to mate with the previously placed lower pouch anchor. The anastomosis formed within 14 days. Due to the tracheobronchial remnant, the device did not pass distally and was removed endoscopically. On postoperative day 8, balloon dilation of the anastomosis and tracheobronchial remnant was performed. Subsequently, the patient required a total of 6 dilations in an 18-month follow-up. This case report illustrates the utility of using magnets to create an esophageal anastomosis in complex cases of EA with concomitant esophageal malformations. The parents of the patient gave their written consent to publish this technical report.</p>","PeriodicalId":43204,"journal":{"name":"European Journal of Pediatric Surgery Reports","volume":"12 1","pages":"e33-e37"},"PeriodicalIF":0.7000,"publicationDate":"2024-02-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10837038/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Pediatric Surgery Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0044-1779042","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
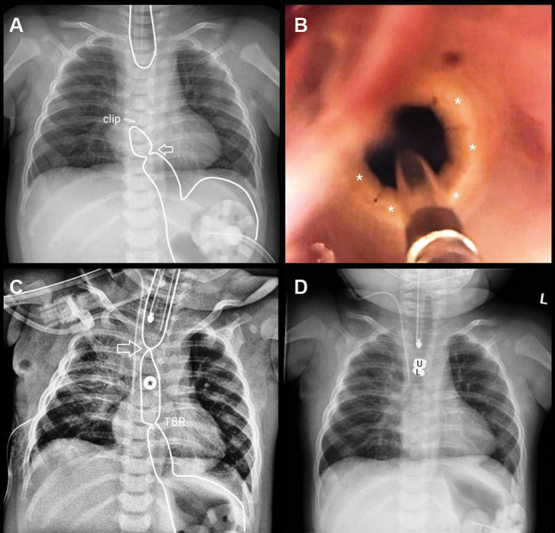
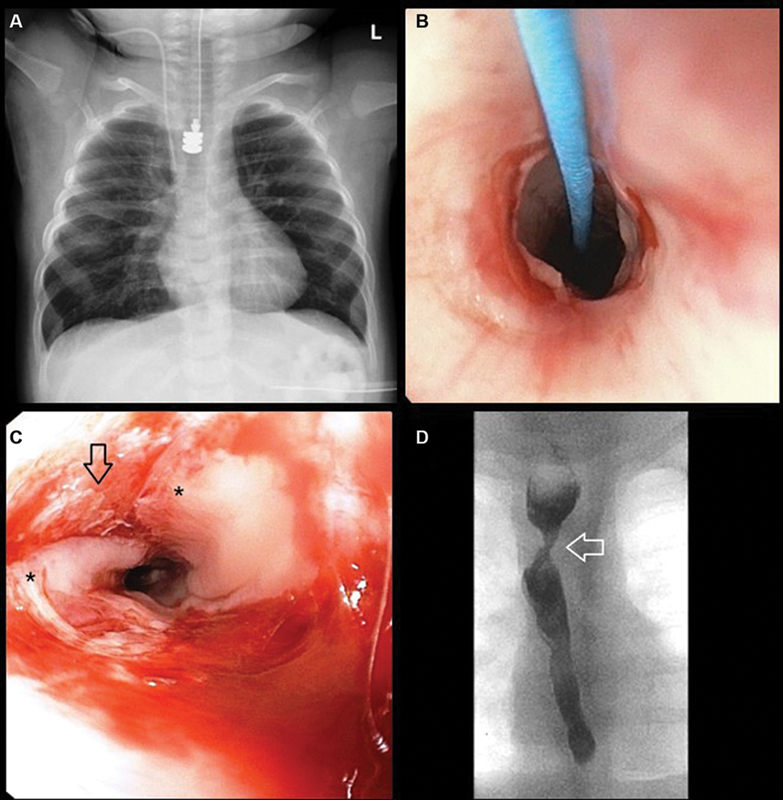
Esophageal atresia (EA) repair can be complicated by associated malformations such as a tracheobronchial remnant in the distal esophagus. We describe our experience with a patient found to have long-gap EA with a distal cartilaginous ring who was managed using a combination of esophageal lengthening and magnetic compression anastomosis. A 5-month-old girl was referred to us from an outside hospital with type C EA including a very high upper pouch. She had undergone a prior thoracotomy with fistula ligation during which a clip was placed on the lower esophagus, leaving a 2-cm diverticulum on the trachea and a short lower esophageal pouch. Upon endoscopic evaluation at our center, we found a tracheobronchial remnant in the lower esophagus between the clip and the carina. An open thoracotomy was performed to approximate the esophageal pouches and a magnet anchor (Connect EA, Myka Laboratories, San Francisco, California, United States) was placed retrograde through the distal esophageal cartilaginous ring into the lower pouch. On postoperative day 8, after adequate growth and decreased pouch tension, a second magnetic anchor was placed endoscopically to the upper pouch to mate with the previously placed lower pouch anchor. The anastomosis formed within 14 days. Due to the tracheobronchial remnant, the device did not pass distally and was removed endoscopically. On postoperative day 8, balloon dilation of the anastomosis and tracheobronchial remnant was performed. Subsequently, the patient required a total of 6 dilations in an 18-month follow-up. This case report illustrates the utility of using magnets to create an esophageal anastomosis in complex cases of EA with concomitant esophageal malformations. The parents of the patient gave their written consent to publish this technical report.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
