Pham-Thi Thao Trang, Tran Chi Cuong, Tran-Thi Thanh Tha, Mai Hoang Dil, Nguyen Manh Cuong, Do Nguyen Tin, Nguyen Tran Tran, Le Minh Thang, Nguyen Duc Chinh, Tran Hoa, Bui The Dung, Tran Ba Hieu, Nguyen Minh Duc
{"title":"A Complicated Case Report of Coronary Artery Fistula.","authors":"Pham-Thi Thao Trang, Tran Chi Cuong, Tran-Thi Thanh Tha, Mai Hoang Dil, Nguyen Manh Cuong, Do Nguyen Tin, Nguyen Tran Tran, Le Minh Thang, Nguyen Duc Chinh, Tran Hoa, Bui The Dung, Tran Ba Hieu, Nguyen Minh Duc","doi":"10.5455/medarh.2023.77.489-492","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Coronary artery fistulas (CAFs), also, known as coronary arteriovenous malformation, are aberrant connections between coronary arteries and other structures, such as other artery branches or heart chambers. CAFs are infrequent and asymptomatic in young patients, but symptoms and complications become more frequent with age. CAFs can affect hemodynamic parameters and lead to complications, such as myocardial ischemia, heart failure, arrhythmia, and infective endocarditis.</p><p><strong>Objective: </strong>The aim of this article was to present a typical CAF case with severe symptoms who underwent successful embolization to resolve their symptoms.</p><p><strong>Case presentation: </strong>A 50-year-old Vietnamese male visited our cardiac outpatient clinic (S.I.S General Hospital, Can Tho, Vietnam) because of exertional dyspnea and chest pain. Signs of congestive heart failure and abnormal murmur were not presented on chest auscultation. Diagnostic digital subtraction angiography was performed to determine the detailed angioarchitecture of the CAF, revealing a fistulous connection between the left anterior descending artery (LAD) and the LV chamber through an aneurysm. In addition, the RCA measured 7 mm in diameter with a fistula (16 × 9 mm) draining into an aneurysm and then terminating into the LV chamber. The patient had an RCA aneurysm with a fistula into the LV. It was treated successfully by closing the fistula with a vascular plug. Access to the fistula was complex and difficult because of complications due to the CAF. After the procedure, the patient had no chest pain or shortness of breath and was discharged after three days. After six months, he was taking dual antiplatelet therapy and antihypertensive medications and felt better. We performed contrast computed tomography (CT) to examine the fistula after a year, which showed the successful closure of the fistula without any relevant alteration in the coronary artery.</p><p><strong>Conclusion: </strong>CAF closure is indicated if patients have symptoms or secondary complications, and percutaneous closure is a safe and effective method to manage CAF. A CAF is rare and does not have specific symptoms, making it difficult to diagnose. Most patients are asymptomatic and have serious recent complications. Currently, the percutaneous transcatheter method is popular because it is noninvasive and successful in most patients.</p>","PeriodicalId":94135,"journal":{"name":"Medical archives (Sarajevo, Bosnia and Herzegovina)","volume":"77 6","pages":"489-492"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10834043/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical archives (Sarajevo, Bosnia and Herzegovina)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5455/medarh.2023.77.489-492","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Coronary artery fistulas (CAFs), also, known as coronary arteriovenous malformation, are aberrant connections between coronary arteries and other structures, such as other artery branches or heart chambers. CAFs are infrequent and asymptomatic in young patients, but symptoms and complications become more frequent with age. CAFs can affect hemodynamic parameters and lead to complications, such as myocardial ischemia, heart failure, arrhythmia, and infective endocarditis.
Objective: The aim of this article was to present a typical CAF case with severe symptoms who underwent successful embolization to resolve their symptoms.
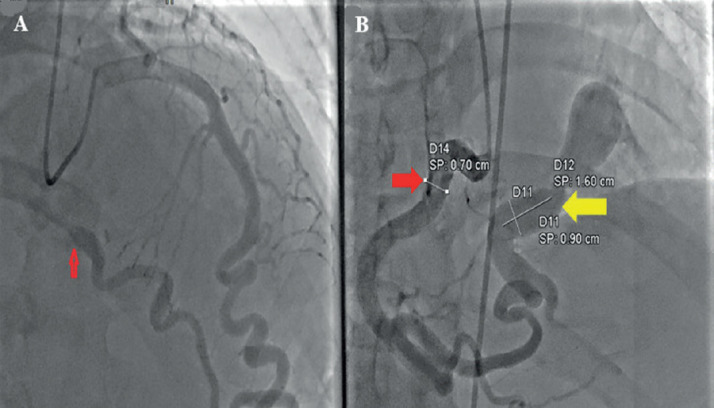
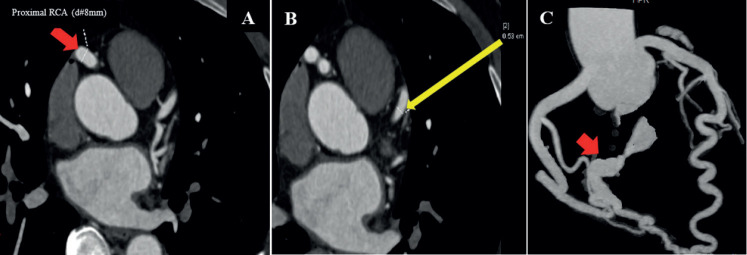
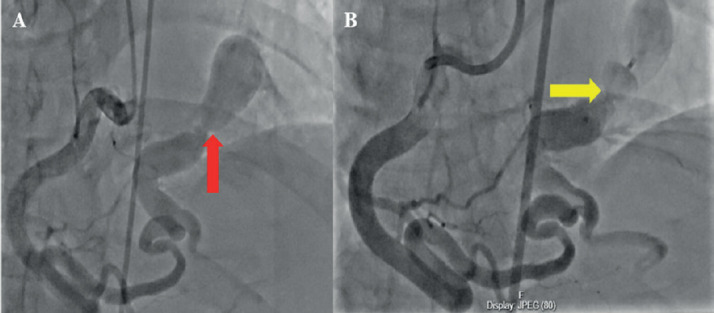
Case presentation: A 50-year-old Vietnamese male visited our cardiac outpatient clinic (S.I.S General Hospital, Can Tho, Vietnam) because of exertional dyspnea and chest pain. Signs of congestive heart failure and abnormal murmur were not presented on chest auscultation. Diagnostic digital subtraction angiography was performed to determine the detailed angioarchitecture of the CAF, revealing a fistulous connection between the left anterior descending artery (LAD) and the LV chamber through an aneurysm. In addition, the RCA measured 7 mm in diameter with a fistula (16 × 9 mm) draining into an aneurysm and then terminating into the LV chamber. The patient had an RCA aneurysm with a fistula into the LV. It was treated successfully by closing the fistula with a vascular plug. Access to the fistula was complex and difficult because of complications due to the CAF. After the procedure, the patient had no chest pain or shortness of breath and was discharged after three days. After six months, he was taking dual antiplatelet therapy and antihypertensive medications and felt better. We performed contrast computed tomography (CT) to examine the fistula after a year, which showed the successful closure of the fistula without any relevant alteration in the coronary artery.
Conclusion: CAF closure is indicated if patients have symptoms or secondary complications, and percutaneous closure is a safe and effective method to manage CAF. A CAF is rare and does not have specific symptoms, making it difficult to diagnose. Most patients are asymptomatic and have serious recent complications. Currently, the percutaneous transcatheter method is popular because it is noninvasive and successful in most patients.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
