{"title":"Antidepressants available in Japan for older people with major depressive disorder: A systematic review and meta-analysis.","authors":"Taro Kishi, Kenji Sakuma, Masakazu Hatano, Takenori Okumura, Masaki Kato, Hajime Baba, Nakao Iwata","doi":"10.1002/npr2.12422","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>To update the major depressive disorder (MDD) treatment guidelines of the Japanese Society of Mood Disorders, we conducted a systematic review and pairwise meta-analysis of double-blind, randomized, placebo-controlled trials of available antidepressants in Japan for older adults with MDD.</p><p><strong>Methods: </strong>Outcome measures included response rate (primary), improvement in depressive symptom scale score, remission rate, all-cause discontinuation, discontinuation due to adverse events, and at least one adverse event. A random-effects model was used to calculate the risk ratio (RR) and standardized mean difference (SMD) with a 95% confidence interval (95% CI).</p><p><strong>Results: </strong>Nine double-blind, randomized, placebo-controlled trials (n = 2145) were identified. No study has been conducted in Japan. Our meta-analysis included the following antidepressants: duloxetine, escitalopram, imipramine, sertraline, venlafaxine, and vortioxetine. Antidepressants have significantly higher response rates than placebo (RR [95% CI] = 1.38 [1.04, 1.83], p = 0.02). Antidepressants outperformed placebo in terms of improving depressive symptom scale score (SMD [95% CI] = -0.62 [-0.92, -0.33], p < 0.0001). However, antidepressants were associated with a higher discontinuation rate due to adverse events (RR [95% CI] = 1.94 [1.30, 2.88], p = 0.001) and a higher incidence of at least one adverse event (RR [95% CI] = 1.11 [1.02, 1.21], p = 0.02) compared to placebo. The groups did not differ significantly in terms of remission rate or all-cause discontinuation.</p><p><strong>Conclusions: </strong>Our meta-analysis concluded that treatment with antidepressants available in Japan is only weakly recommended for moderate to severe MDD in older adults.</p>","PeriodicalId":19137,"journal":{"name":"Neuropsychopharmacology Reports","volume":" ","pages":"267-271"},"PeriodicalIF":2.0000,"publicationDate":"2024-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10932767/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neuropsychopharmacology Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/npr2.12422","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/6 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"NEUROSCIENCES","Score":null,"Total":0}
引用次数: 0
Abstract
Aim: To update the major depressive disorder (MDD) treatment guidelines of the Japanese Society of Mood Disorders, we conducted a systematic review and pairwise meta-analysis of double-blind, randomized, placebo-controlled trials of available antidepressants in Japan for older adults with MDD.
Methods: Outcome measures included response rate (primary), improvement in depressive symptom scale score, remission rate, all-cause discontinuation, discontinuation due to adverse events, and at least one adverse event. A random-effects model was used to calculate the risk ratio (RR) and standardized mean difference (SMD) with a 95% confidence interval (95% CI).
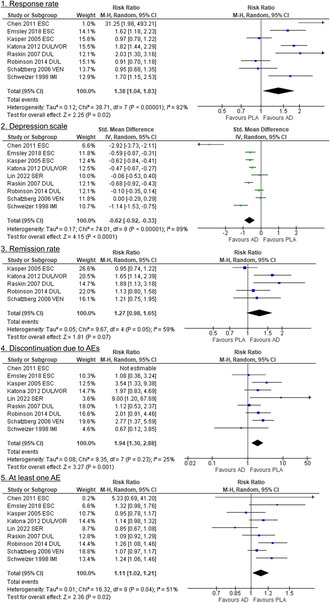
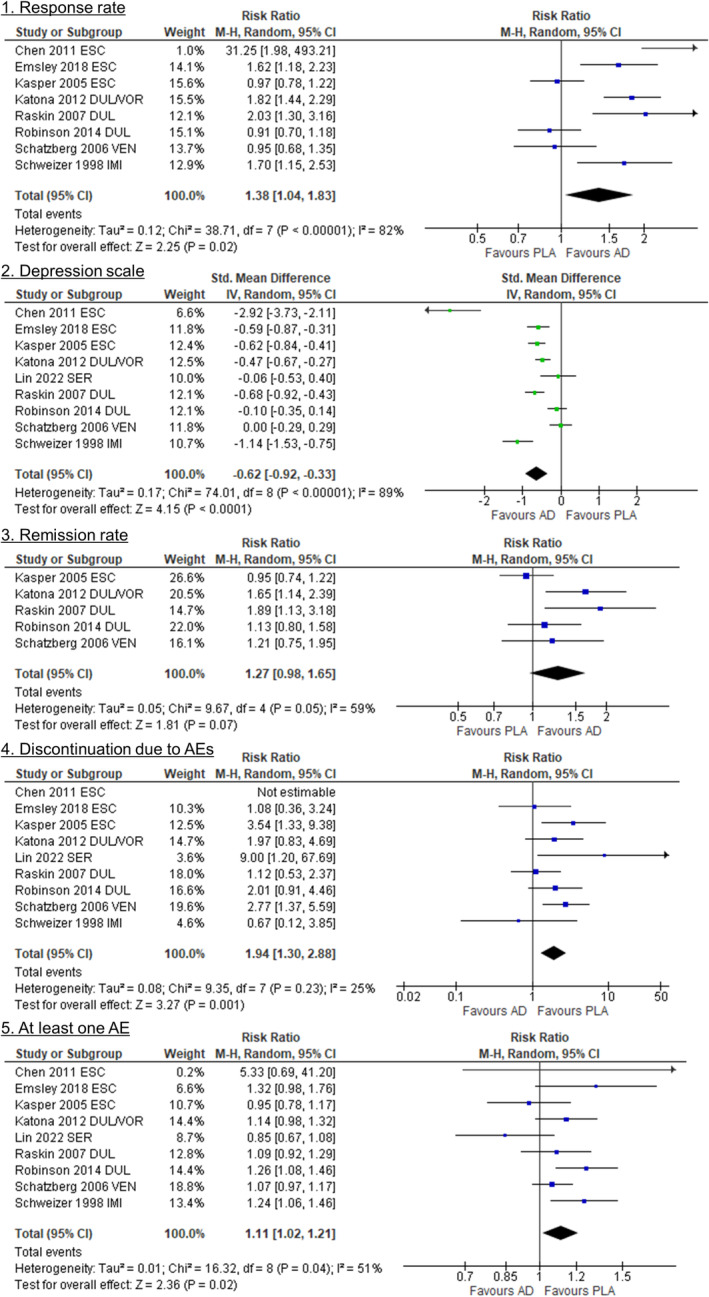
Results: Nine double-blind, randomized, placebo-controlled trials (n = 2145) were identified. No study has been conducted in Japan. Our meta-analysis included the following antidepressants: duloxetine, escitalopram, imipramine, sertraline, venlafaxine, and vortioxetine. Antidepressants have significantly higher response rates than placebo (RR [95% CI] = 1.38 [1.04, 1.83], p = 0.02). Antidepressants outperformed placebo in terms of improving depressive symptom scale score (SMD [95% CI] = -0.62 [-0.92, -0.33], p < 0.0001). However, antidepressants were associated with a higher discontinuation rate due to adverse events (RR [95% CI] = 1.94 [1.30, 2.88], p = 0.001) and a higher incidence of at least one adverse event (RR [95% CI] = 1.11 [1.02, 1.21], p = 0.02) compared to placebo. The groups did not differ significantly in terms of remission rate or all-cause discontinuation.
Conclusions: Our meta-analysis concluded that treatment with antidepressants available in Japan is only weakly recommended for moderate to severe MDD in older adults.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
