Shuaibo Wang, Xujie Sun, Jiyan Dong, Li Liu, Hao Zhao, Renda Li, Zhenlin Yang, Na Cheng, Yalong Wang, Li Fu, Hang Yi, Zhuoheng Lv, Huandong Huo, Donghui Jin, Yousheng Mao, Lin Yang
{"title":"Pathological response and tumor stroma immunogenic features predict long-term survival in non-small cell lung cancer after neoadjuvant chemotherapy.","authors":"Shuaibo Wang, Xujie Sun, Jiyan Dong, Li Liu, Hao Zhao, Renda Li, Zhenlin Yang, Na Cheng, Yalong Wang, Li Fu, Hang Yi, Zhuoheng Lv, Huandong Huo, Donghui Jin, Yousheng Mao, Lin Yang","doi":"10.1007/s13402-023-00914-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Major pathological response (MPR) has become a surrogate endpoint for overall survival (OS) in non-small cell lung cancer (NSCLC) after neoadjuvant therapy, however, the prognostic histologic features and optimal N descriptor after neoadjuvant therapy are poorly defined.</p><p><strong>Methods: </strong>We retrospectively analyzed data from 368 NSCLC patients who underwent surgery after neoadjuvant chemotherapy (NAC) from January 2010 to December 2020. The percentage of residual viable tumors in the primary tumor, lymph nodes (LN), and inflammation components within the tumor stroma were comprehensively reviewed. The primary endpoint was OS.</p><p><strong>Results: </strong>Of the 368 enrolled patients, 12.0% (44/368) achieved MPR in the primary tumor, which was associated with significantly better OS (HR, 0.36 0.17-0.77, p = 0.008) and DFS (HR = 0.59, 0.36-0.92, p = 0.038). In patients who did not have an MPR, we identified an immune-activated phenotype in primary tumors, characterized by intense tumor-infiltrating lymphocyte or multinucleated giant cell infiltration, that was associated with similar OS and DFS as patients who had MPR. Neoadjuvant pathologic grade (NPG), consisting of MPR and immune-activated phenotype, identified 30.7% (113/368) patients that derived significant OS (HR 0.28, 0.17-0.46, p < 0.001) and DFS (HR 0.44, 0.31-0.61, p < 0.001) benefit from NAC. Moreover, the combination of NPG and the number of positive LN stations (nS) in the multivariate analysis had a higher C-index (0.711 vs. 0.663, p < 0.001) than the ypTNM Stage when examining OS.</p><p><strong>Conclusion: </strong>NPG integrated with nS can provide a simple, practical, and robust approach that may allow for better stratification of patients when evaluating neoadjuvant chemotherapy in clinical practice.</p>","PeriodicalId":49223,"journal":{"name":"Cellular Oncology","volume":" ","pages":"1005-1024"},"PeriodicalIF":4.8000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12974087/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cellular Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s13402-023-00914-6","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/6 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CELL BIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Major pathological response (MPR) has become a surrogate endpoint for overall survival (OS) in non-small cell lung cancer (NSCLC) after neoadjuvant therapy, however, the prognostic histologic features and optimal N descriptor after neoadjuvant therapy are poorly defined.
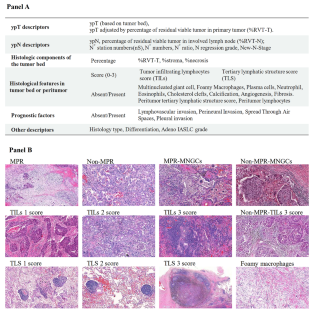
Methods: We retrospectively analyzed data from 368 NSCLC patients who underwent surgery after neoadjuvant chemotherapy (NAC) from January 2010 to December 2020. The percentage of residual viable tumors in the primary tumor, lymph nodes (LN), and inflammation components within the tumor stroma were comprehensively reviewed. The primary endpoint was OS.
Results: Of the 368 enrolled patients, 12.0% (44/368) achieved MPR in the primary tumor, which was associated with significantly better OS (HR, 0.36 0.17-0.77, p = 0.008) and DFS (HR = 0.59, 0.36-0.92, p = 0.038). In patients who did not have an MPR, we identified an immune-activated phenotype in primary tumors, characterized by intense tumor-infiltrating lymphocyte or multinucleated giant cell infiltration, that was associated with similar OS and DFS as patients who had MPR. Neoadjuvant pathologic grade (NPG), consisting of MPR and immune-activated phenotype, identified 30.7% (113/368) patients that derived significant OS (HR 0.28, 0.17-0.46, p < 0.001) and DFS (HR 0.44, 0.31-0.61, p < 0.001) benefit from NAC. Moreover, the combination of NPG and the number of positive LN stations (nS) in the multivariate analysis had a higher C-index (0.711 vs. 0.663, p < 0.001) than the ypTNM Stage when examining OS.
Conclusion: NPG integrated with nS can provide a simple, practical, and robust approach that may allow for better stratification of patients when evaluating neoadjuvant chemotherapy in clinical practice.
期刊介绍:
The Official Journal of the International Society for Cellular Oncology
Focuses on translational research
Addresses the conversion of cell biology to clinical applications
Cellular Oncology publishes scientific contributions from various biomedical and clinical disciplines involved in basic and translational cancer research on the cell and tissue level, technical and bioinformatics developments in this area, and clinical applications. This includes a variety of fields like genome technology, micro-arrays and other high-throughput techniques, genomic instability, SNP, DNA methylation, signaling pathways, DNA organization, (sub)microscopic imaging, proteomics, bioinformatics, functional effects of genomics, drug design and development, molecular diagnostics and targeted cancer therapies, genotype-phenotype interactions.
A major goal is to translate the latest developments in these fields from the research laboratory into routine patient management. To this end Cellular Oncology forms a platform of scientific information exchange between molecular biologists and geneticists, technical developers, pathologists, (medical) oncologists and other clinicians involved in the management of cancer patients.
In vitro studies are preferentially supported by validations in tumor tissue with clinicopathological associations.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
