Vincenza Conteduca, Piergiorgio Di Tullio, Rossana Allamprese, Giuseppina Bruno, Cristian Lolli, Giuseppe Schepisi, Aldo Rosano, Guido Giordano, Marianna Garofoli, Vincenzo Emanuele Chiuri, Lucia Fratino, Elisa Zanardi, Luca Galli, Francesco Massari, Ugo Falagario, Pasquale Rescigno, Giuseppe Fornarini, Francesca Sanguedolce, Daniele Santini, Giuseppe Procopio, Orazio Caffo, Giuseppe Carrieri, Matteo Landriscina, Ugo De Giorgi
{"title":"Initial management approach for localized/locally advanced disease is critical to guide metastatic castration-resistant prostate cancer care","authors":"Vincenza Conteduca, Piergiorgio Di Tullio, Rossana Allamprese, Giuseppina Bruno, Cristian Lolli, Giuseppe Schepisi, Aldo Rosano, Guido Giordano, Marianna Garofoli, Vincenzo Emanuele Chiuri, Lucia Fratino, Elisa Zanardi, Luca Galli, Francesco Massari, Ugo Falagario, Pasquale Rescigno, Giuseppe Fornarini, Francesca Sanguedolce, Daniele Santini, Giuseppe Procopio, Orazio Caffo, Giuseppe Carrieri, Matteo Landriscina, Ugo De Giorgi","doi":"10.1038/s41391-024-00800-8","DOIUrl":null,"url":null,"abstract":"Currently, several therapies are available for metastatic castration-resistant prostate cancer (mCRPC) but no specific clinical factors to personalize treatment. We first sought the prognostic value of duration on androgen-deprivation therapy (ADT) for hormone-sensitive prostate cancer (HSPC) in patients receiving androgen-receptor-signaling inhibitors (ARSI) for mCRPC. A multicenter cohort of mCRPC patients who started ARSI between July 2011 and October 2021 was identified. Based on their initial disease burden and duration on ADT for HSPC, primary progressive (PP) men were classified into four groups: low/intermediate-risk localized disease (LOC) and high-risk localized/locally advanced disease (LAD) and short-term (ST) < 24 vs. long-term (LT) ADT ≥ 24 months, whereas de novo (DN) mHSPC were subdivided into short-time vs. long-time to CRPC. We included 919 mCRPC patients with a median age of 77 years [interquartile range (IQR) = 71–82)]. Median ADT duration in HSPC was 24 months (IQR = 14–40). Median follow-up was 91 months (IQR = 62–138), median OS and PFS from ARSI start were 20 (IQR 10–32) and 10 months (IQR = 5–19), respectively. In PP developing metastatic disease (n = 655, 71.3%), LOC and LAD with ST ADT had a greater than almost double-risk of death compared to LT ADT (LOC/ST: hazard ratio [HR] = 2.01; 95% CI 1.54–2.64; LAD/ST: HR = 1.73; 95% CI 1.34–2.24; p < 0.001). In the multivariate analysis including age, prognostic cohort, Gleason, ECOG, radical radiotherapy and prostatectomy, groups with ST ADT were associated with worse OS compared to LT ADT (LOC/ST: HR = 1.84; 95% CI 1.38–2.45; p < 0.001; LAD/ST: HR = 1.59; 95% CI 1.21–2.10; p < 0.001), along with ECOG > 2 (HR = 1.55; 95% CI 1.06–2.26; p = 0.03). There were also similar results of PFS. Moreover, long-time to CRPC in patients with history of DN mHSPC (n = 264, 28.7%) resulted in a better OS/PFS (HR = 0.76, 95% CI 0.56–1.02, p = 0.064 and HR = 0.74, 95% CI 0.55–0.99, p = 0.042, respectively). Our study showed that duration on ADT for mHSPC was significantly associated with survival in mCRPC undergoing ARSI. These findings suggest a possible connection between initial management of prostate tumour and a better prognostication in mCRPC. Prospective trials are warranted.","PeriodicalId":20727,"journal":{"name":"Prostate Cancer and Prostatic Diseases","volume":"28 2","pages":"370-377"},"PeriodicalIF":5.8000,"publicationDate":"2024-02-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Prostate Cancer and Prostatic Diseases","FirstCategoryId":"3","ListUrlMain":"https://www.nature.com/articles/s41391-024-00800-8","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
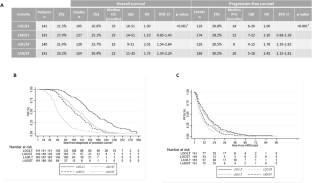
Currently, several therapies are available for metastatic castration-resistant prostate cancer (mCRPC) but no specific clinical factors to personalize treatment. We first sought the prognostic value of duration on androgen-deprivation therapy (ADT) for hormone-sensitive prostate cancer (HSPC) in patients receiving androgen-receptor-signaling inhibitors (ARSI) for mCRPC. A multicenter cohort of mCRPC patients who started ARSI between July 2011 and October 2021 was identified. Based on their initial disease burden and duration on ADT for HSPC, primary progressive (PP) men were classified into four groups: low/intermediate-risk localized disease (LOC) and high-risk localized/locally advanced disease (LAD) and short-term (ST) < 24 vs. long-term (LT) ADT ≥ 24 months, whereas de novo (DN) mHSPC were subdivided into short-time vs. long-time to CRPC. We included 919 mCRPC patients with a median age of 77 years [interquartile range (IQR) = 71–82)]. Median ADT duration in HSPC was 24 months (IQR = 14–40). Median follow-up was 91 months (IQR = 62–138), median OS and PFS from ARSI start were 20 (IQR 10–32) and 10 months (IQR = 5–19), respectively. In PP developing metastatic disease (n = 655, 71.3%), LOC and LAD with ST ADT had a greater than almost double-risk of death compared to LT ADT (LOC/ST: hazard ratio [HR] = 2.01; 95% CI 1.54–2.64; LAD/ST: HR = 1.73; 95% CI 1.34–2.24; p < 0.001). In the multivariate analysis including age, prognostic cohort, Gleason, ECOG, radical radiotherapy and prostatectomy, groups with ST ADT were associated with worse OS compared to LT ADT (LOC/ST: HR = 1.84; 95% CI 1.38–2.45; p < 0.001; LAD/ST: HR = 1.59; 95% CI 1.21–2.10; p < 0.001), along with ECOG > 2 (HR = 1.55; 95% CI 1.06–2.26; p = 0.03). There were also similar results of PFS. Moreover, long-time to CRPC in patients with history of DN mHSPC (n = 264, 28.7%) resulted in a better OS/PFS (HR = 0.76, 95% CI 0.56–1.02, p = 0.064 and HR = 0.74, 95% CI 0.55–0.99, p = 0.042, respectively). Our study showed that duration on ADT for mHSPC was significantly associated with survival in mCRPC undergoing ARSI. These findings suggest a possible connection between initial management of prostate tumour and a better prognostication in mCRPC. Prospective trials are warranted.
期刊介绍:
Prostate Cancer and Prostatic Diseases covers all aspects of prostatic diseases, in particular prostate cancer, the subject of intensive basic and clinical research world-wide. The journal also reports on exciting new developments being made in diagnosis, surgery, radiotherapy, drug discovery and medical management.
Prostate Cancer and Prostatic Diseases is of interest to surgeons, oncologists and clinicians treating patients and to those involved in research into diseases of the prostate. The journal covers the three main areas - prostate cancer, male LUTS and prostatitis.
Prostate Cancer and Prostatic Diseases publishes original research articles, reviews, topical comment and critical appraisals of scientific meetings and the latest books. The journal also contains a calendar of forthcoming scientific meetings. The Editors and a distinguished Editorial Board ensure that submitted articles receive fast and efficient attention and are refereed to the highest possible scientific standard. A fast track system is available for topical articles of particular significance.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
