Theresa Frank, Jens Neumann, Anne Assmann, Stefanie Schreiber, Aiden Haghikia, Maria Barleben, Michael Sailer, Michael Goertler
{"title":"Predictors for Adherence to Recommended Anticoagulation after Stroke Unit Discharge in Patients with Atrial Fibrillation.","authors":"Theresa Frank, Jens Neumann, Anne Assmann, Stefanie Schreiber, Aiden Haghikia, Maria Barleben, Michael Sailer, Michael Goertler","doi":"10.1159/000537781","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Non-adherence to recommended secondary preventive anticoagulation in stroke patients with atrial fibrillation (AF) is a common phenomenon although the introduction of direct oral anticoagulants (DOACs) has simplified anticoagulation management for physicians as well as for patients.</p><p><strong>Methods: </strong>We examined the adherence of secondary preventive anticoagulation in AF patients after re-integration in their social environment 6 to 12 weeks after stroke unit and rehabilitation clinic treatment and analyzed for predictors for adherence and non-adherence. We conducted a telephone survey in consecutive patients treated between January 2013 and December 2021 at our institutional stroke unit with an acute cerebrovascular ischemic event and we analyzed discharge letters of rehabilitation clinics of those patients not anticoagulated at follow-up. All patients had known or newly diagnosed AF and in all we had recommended secondary preventive anticoagulation.</p><p><strong>Results: </strong>Follow-up information about anticoagulant intake could be obtained in 1348 of 1685 patients (80.0%) treated within the study period. Anticoagulation rate was 91.5% with 83.6% of patients receiving DOACs and 7.9% receiving vitamin K antagonists (VKAs). Adherence to recommended anticoagulation was associated with intake of the recommended anticoagulant already at discharge (adjusted OR, 18.357; CI, 9.637 to 34.969), recommendation of a specific DOAC and dose (in contrast to \"DOAC\" as drug category) (adjusted OR, 2.971; CI, 1.173 to 7.255), a lower modified Rankin Scale at discharge (per point; adjusted OR, 0.813; CI, 0.663 to 0.996), younger age (per year; adjusted odds ratio [OR], 0.951; confidence interval [CI], 0.926 to 0.976), and the absence of peripheral vascular disease (adjusted OR, 0.359; CI, 0.173 to 0.746). In patients already anticoagulated at discharge adherence was 98.5%, irrespective of a patient's age, functional deficit at discharge, and peripheral vascular disease. Avoidable obstacles for non-adherence in patients not on anticoagulants at stroke unit discharge were (1) non-implementation of recommended anticoagulation by rehabilitation physicians predominantly in patients with moderate-severe or severe stroke disability (2.1%), (2) delegation of anticoagulation start from rehabilitation physicians to general practitioners/resident radiologists (1.3%), and (3) rejection of recommended anticoagulation because of patients' severe stroke disability (0.5%). Non-avoidable obstacles were contraindications to anticoagulation (2.1%) and patients' refusal (0.7%).</p><p><strong>Conclusions: </strong>Commencing drug administration already during stroke unit hospitalization and providing an explanation for the selection of the recommended anticoagulant in discharge letters ensures high adherence at patients' re-integration in their social environment after acute stroke treatment. If drug administration cannot be commenced before discharge, education of rehabilitation physicians by stroke physicians and the involvement of stroke physicians into the post-stroke decision process might hinder avoidable obstacles.</p>","PeriodicalId":45709,"journal":{"name":"Cerebrovascular Diseases Extra","volume":" ","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2024-02-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10923591/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cerebrovascular Diseases Extra","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000537781","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Non-adherence to recommended secondary preventive anticoagulation in stroke patients with atrial fibrillation (AF) is a common phenomenon although the introduction of direct oral anticoagulants (DOACs) has simplified anticoagulation management for physicians as well as for patients.
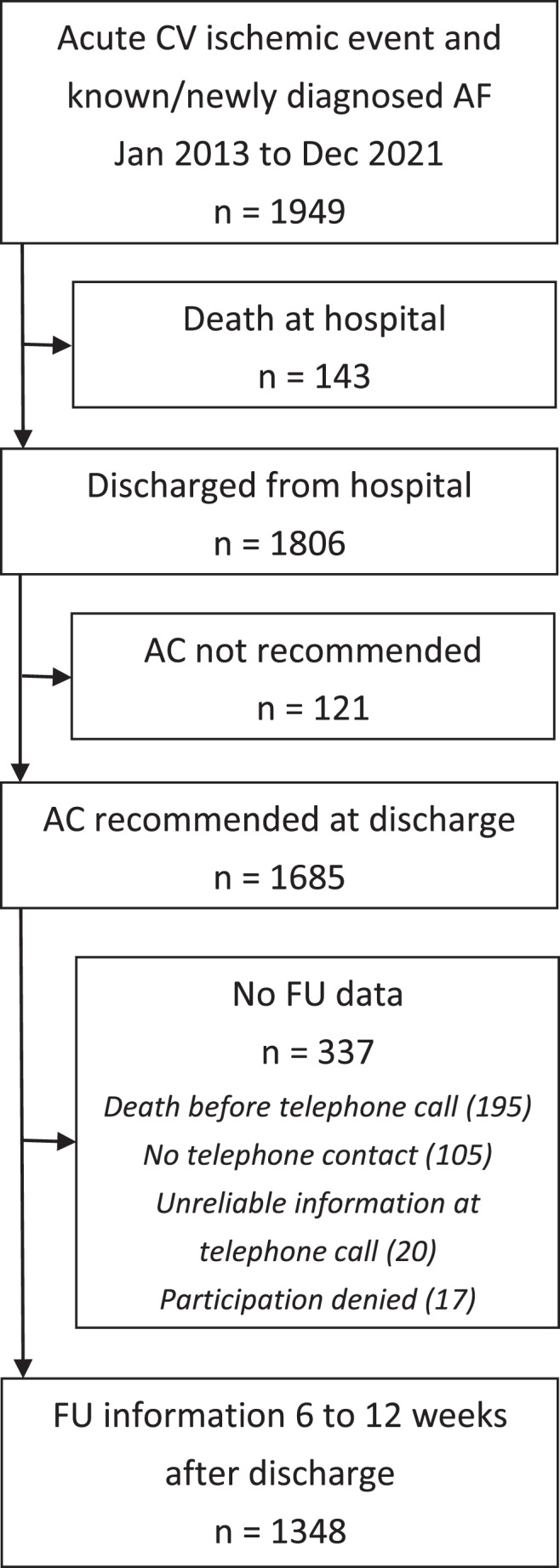
Methods: We examined the adherence of secondary preventive anticoagulation in AF patients after re-integration in their social environment 6 to 12 weeks after stroke unit and rehabilitation clinic treatment and analyzed for predictors for adherence and non-adherence. We conducted a telephone survey in consecutive patients treated between January 2013 and December 2021 at our institutional stroke unit with an acute cerebrovascular ischemic event and we analyzed discharge letters of rehabilitation clinics of those patients not anticoagulated at follow-up. All patients had known or newly diagnosed AF and in all we had recommended secondary preventive anticoagulation.
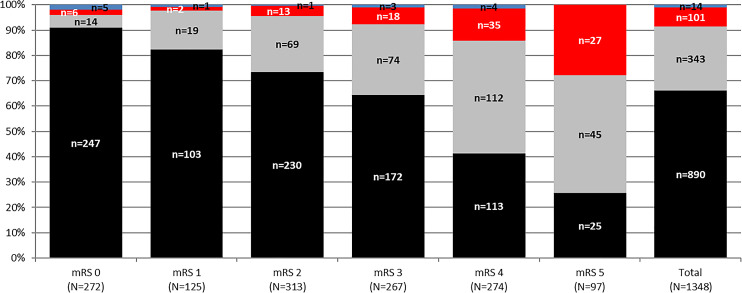
Results: Follow-up information about anticoagulant intake could be obtained in 1348 of 1685 patients (80.0%) treated within the study period. Anticoagulation rate was 91.5% with 83.6% of patients receiving DOACs and 7.9% receiving vitamin K antagonists (VKAs). Adherence to recommended anticoagulation was associated with intake of the recommended anticoagulant already at discharge (adjusted OR, 18.357; CI, 9.637 to 34.969), recommendation of a specific DOAC and dose (in contrast to "DOAC" as drug category) (adjusted OR, 2.971; CI, 1.173 to 7.255), a lower modified Rankin Scale at discharge (per point; adjusted OR, 0.813; CI, 0.663 to 0.996), younger age (per year; adjusted odds ratio [OR], 0.951; confidence interval [CI], 0.926 to 0.976), and the absence of peripheral vascular disease (adjusted OR, 0.359; CI, 0.173 to 0.746). In patients already anticoagulated at discharge adherence was 98.5%, irrespective of a patient's age, functional deficit at discharge, and peripheral vascular disease. Avoidable obstacles for non-adherence in patients not on anticoagulants at stroke unit discharge were (1) non-implementation of recommended anticoagulation by rehabilitation physicians predominantly in patients with moderate-severe or severe stroke disability (2.1%), (2) delegation of anticoagulation start from rehabilitation physicians to general practitioners/resident radiologists (1.3%), and (3) rejection of recommended anticoagulation because of patients' severe stroke disability (0.5%). Non-avoidable obstacles were contraindications to anticoagulation (2.1%) and patients' refusal (0.7%).
Conclusions: Commencing drug administration already during stroke unit hospitalization and providing an explanation for the selection of the recommended anticoagulant in discharge letters ensures high adherence at patients' re-integration in their social environment after acute stroke treatment. If drug administration cannot be commenced before discharge, education of rehabilitation physicians by stroke physicians and the involvement of stroke physicians into the post-stroke decision process might hinder avoidable obstacles.
期刊介绍:
This open access and online-only journal publishes original articles covering the entire spectrum of stroke and cerebrovascular research, drawing from a variety of specialties such as neurology, internal medicine, surgery, radiology, epidemiology, cardiology, hematology, psychology and rehabilitation. Offering an international forum, it meets the growing need for sophisticated, up-to-date scientific information on clinical data, diagnostic testing, and therapeutic issues. The journal publishes original contributions, reviews of selected topics as well as clinical investigative studies. All aspects related to clinical advances are considered, while purely experimental work appears only if directly relevant to clinical issues. Cerebrovascular Diseases Extra provides additional contents based on reviewed and accepted submissions to the main journal Cerebrovascular Diseases.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
