External validation of the HACOR score and ROX index for predicting treatment failure in patients with coronavirus disease 2019 pneumonia managed on high-flow nasal cannula therapy: a multicenter retrospective observational study in Japan.
{"title":"External validation of the HACOR score and ROX index for predicting treatment failure in patients with coronavirus disease 2019 pneumonia managed on high-flow nasal cannula therapy: a multicenter retrospective observational study in Japan.","authors":"Hiromu Okano, Ryohei Yamamoto, Yudai Iwasaki, Daisuke Irimada, Daisuke Konno, Taku Tanaka, Takatoshi Oishi, Hiroki Nawa, Akihiko Yano, Hiroaki Taniguchi, Masayuki Otawara, Ayaka Matsuoka, Masanori Yamauchi","doi":"10.1186/s40560-024-00720-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The HACOR score for predicting treatment failure includes vital signs and acid-base balance factors, whereas the ROX index only considers the respiratory rate, oxygen saturation, and fraction of inspired oxygen (FiO<sub>2</sub>). We aimed to externally validate the HACOR score and ROX index for predicting treatment failure in patients with coronavirus disease 2019 (COVID-19) on high-flow nasal cannula (HFNC) therapy in Japan.</p><p><strong>Methods: </strong>This retrospective, observational, multicenter study included patients, aged ≥ 18 years, diagnosed with COVID-19 and treated with HFNC therapy between January 16, 2020, and March 31, 2022. The HACOR score and ROX index were calculated at 2, 6, 12, 24, and 48 h after stating HFNC therapy. The primary outcome was treatment failure (requirement for intubation or occurrence of death within 7 days). We calculated the area under the receiver operating characteristic curve (AUROC) and assessed the diagnostic performance of these indicators. The 2-h time-point prediction was considered the primary analysis and that of other time-points as the secondary analysis. We also assessed 2-h time-point sensitivity and specificity using previously reported cutoff values (HACOR score > 5, ROX index < 2.85).</p><p><strong>Results: </strong>We analyzed 300 patients from 9 institutions (median age, 60 years; median SpO<sub>2</sub>/FiO<sub>2</sub> ratio at the start of HFNC therapy, 121). Within 7 days of HFNC therapy, treatment failure occurred in 127 (42%) patients. The HACOR score and ROX index at the 2-h time-point exhibited AUROC discrimination values of 0.63 and 0.57 (P = 0.24), respectively. These values varied with temporal changes-0.58 and 0.62 at 6 h, 0.70 and 0.68 at 12 h, 0.68 and 0.69 at 24 h, and 0.75 and 0.75 at 48 h, respectively. The 2-h time-point sensitivity and specificity were 18% and 91% for the HACOR score, respectively, and 3% and 100% for the ROX index, respectively. Visual calibration assessment revealed well calibrated HACOR score, but not ROX index.</p><p><strong>Conclusions: </strong>In COVID-19 patients receiving HFNC therapy in Japan, the predictive performance of the HACOR score and ROX index at the 2-h time-point may be inadequate. Furthermore, clinicians should be mindful of time-point scores owing to the variation of the models' predictive performance with the time-point. Trial registration UMIN (registration number: UMIN000050024, January 13, 2023).</p>","PeriodicalId":16123,"journal":{"name":"Journal of Intensive Care","volume":"12 1","pages":"7"},"PeriodicalIF":4.7000,"publicationDate":"2024-02-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10870626/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40560-024-00720-8","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
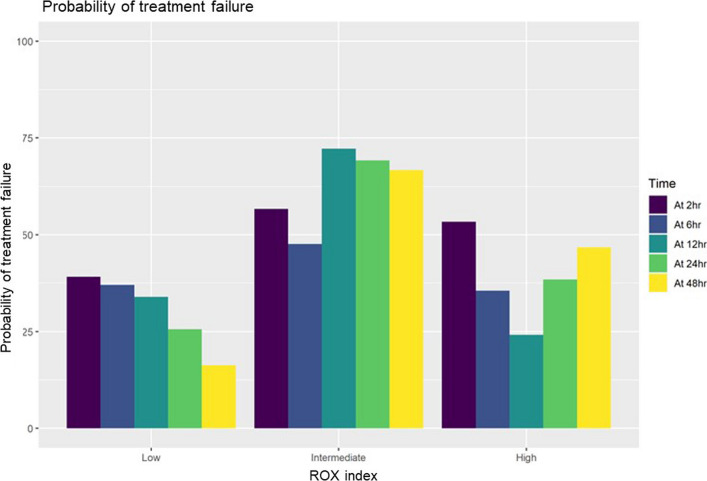
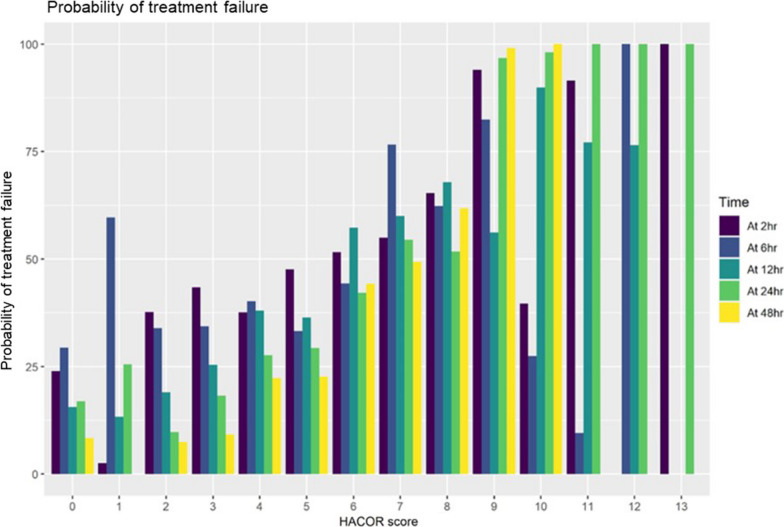
Background: The HACOR score for predicting treatment failure includes vital signs and acid-base balance factors, whereas the ROX index only considers the respiratory rate, oxygen saturation, and fraction of inspired oxygen (FiO2). We aimed to externally validate the HACOR score and ROX index for predicting treatment failure in patients with coronavirus disease 2019 (COVID-19) on high-flow nasal cannula (HFNC) therapy in Japan.
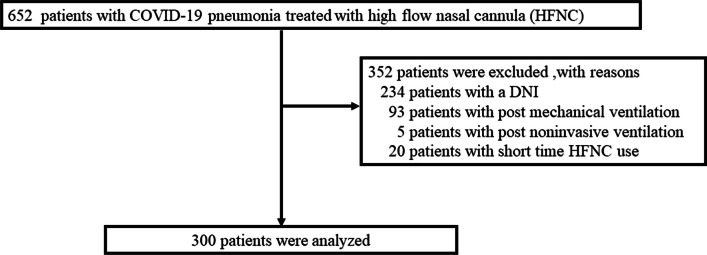
Methods: This retrospective, observational, multicenter study included patients, aged ≥ 18 years, diagnosed with COVID-19 and treated with HFNC therapy between January 16, 2020, and March 31, 2022. The HACOR score and ROX index were calculated at 2, 6, 12, 24, and 48 h after stating HFNC therapy. The primary outcome was treatment failure (requirement for intubation or occurrence of death within 7 days). We calculated the area under the receiver operating characteristic curve (AUROC) and assessed the diagnostic performance of these indicators. The 2-h time-point prediction was considered the primary analysis and that of other time-points as the secondary analysis. We also assessed 2-h time-point sensitivity and specificity using previously reported cutoff values (HACOR score > 5, ROX index < 2.85).
Results: We analyzed 300 patients from 9 institutions (median age, 60 years; median SpO2/FiO2 ratio at the start of HFNC therapy, 121). Within 7 days of HFNC therapy, treatment failure occurred in 127 (42%) patients. The HACOR score and ROX index at the 2-h time-point exhibited AUROC discrimination values of 0.63 and 0.57 (P = 0.24), respectively. These values varied with temporal changes-0.58 and 0.62 at 6 h, 0.70 and 0.68 at 12 h, 0.68 and 0.69 at 24 h, and 0.75 and 0.75 at 48 h, respectively. The 2-h time-point sensitivity and specificity were 18% and 91% for the HACOR score, respectively, and 3% and 100% for the ROX index, respectively. Visual calibration assessment revealed well calibrated HACOR score, but not ROX index.
Conclusions: In COVID-19 patients receiving HFNC therapy in Japan, the predictive performance of the HACOR score and ROX index at the 2-h time-point may be inadequate. Furthermore, clinicians should be mindful of time-point scores owing to the variation of the models' predictive performance with the time-point. Trial registration UMIN (registration number: UMIN000050024, January 13, 2023).
期刊介绍:
"Journal of Intensive Care" is an open access journal dedicated to the comprehensive coverage of intensive care medicine, providing a platform for the latest research and clinical insights in this critical field. The journal covers a wide range of topics, including intensive and critical care, trauma and surgical intensive care, pediatric intensive care, acute and emergency medicine, perioperative medicine, resuscitation, infection control, and organ dysfunction.
Recognizing the importance of cultural diversity in healthcare practices, "Journal of Intensive Care" also encourages submissions that explore and discuss the cultural aspects of intensive care, aiming to promote a more inclusive and culturally sensitive approach to patient care. By fostering a global exchange of knowledge and expertise, the journal contributes to the continuous improvement of intensive care practices worldwide.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
