Aloysius Ugwu-Olisa Ogbuanya, Uche Emmanuel Eni, Daniel A Umezurike, Akputa A Obasi, Somadina Ikpeze
{"title":"Associated Factors of Leaked Repair Following Omentopexy for Perforated Peptic Ulcer Disease; a Cross-sectional Study.","authors":"Aloysius Ugwu-Olisa Ogbuanya, Uche Emmanuel Eni, Daniel A Umezurike, Akputa A Obasi, Somadina Ikpeze","doi":"10.22037/aaem.v12i1.2169","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Previous studies have reported numerous clinico-pathologic risk factors associated with increased risk of leaked repair following omental patch for perforated peptic ulcer disease (PPUD). This study aimed to analyze the risk factors associated with leaked repair of omental patch and document the management and outcome of established cases of leaked repair in a resource-poor setting.</p><p><strong>Methods: </strong>This is a multicenter cross-sectional study of leaked repair after omental patch of PPUD between January 2016 to December 2022. Following primary repair of PPUD with omental pedicle reinforcement, associated factors of leaked repair were evaluated using univariate and multivariate analyses.</p><p><strong>Results: </strong>Overall, 360 cases were evaluated (62.8% male). Leaked repair rate was 11.7% (42 cases). Those without immunosuppression were 3 times less likely to have leaked repair (aOR= 0.34; 95% CI: 0.16 - 0.72; p = 0.003) while those with sepsis were 4 times more likely to have leaked repair (aOR=4.16; 95% CI: 1.06 - 12.36; p = 0.018). Patients with delayed presentation (>48 hours) were 2.5 times more likely to have leaked repair than those who presented in 0 - 24 hours (aOR=2.51; 95% CI: 3.62 - 10.57; p = 0.044). Those with Perforation diameter 2.1-3.0 cm were 8 times (aOR=7.98; 95% CI: 2.63-24.21; p<0.0001), and those with perforation diameter > 3.0cm were 33 times (aOR=33.04; 95% CI: 10.98-100.25; p<0.0001) more likely to have leaked repair than those with perforation diameter of 0-1.0 cm. Similarly, in those with no perioperative shock, leaked repair was 4 times less likely to develop than those with perioperative shock (aOR= 0.42; 95% CI: 0.41-0.92; p = 0.041). There was significant statistical difference in morbidity (p = 0.003) and mortality (p < 0.0001) rates for cases of leaked repairs and successful repairs.</p><p><strong>Conclusion: </strong>Leaked repair following omentopexy for peptic ulcer perforation was significantly associated with large perforation diameter, delayed presentation, sepsis, immunosuppressive therapy, and perioperative shock.</p>","PeriodicalId":8146,"journal":{"name":"Archives of Academic Emergency Medicine","volume":"12 1","pages":"e18"},"PeriodicalIF":2.0000,"publicationDate":"2023-12-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10871054/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archives of Academic Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22037/aaem.v12i1.2169","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Previous studies have reported numerous clinico-pathologic risk factors associated with increased risk of leaked repair following omental patch for perforated peptic ulcer disease (PPUD). This study aimed to analyze the risk factors associated with leaked repair of omental patch and document the management and outcome of established cases of leaked repair in a resource-poor setting.
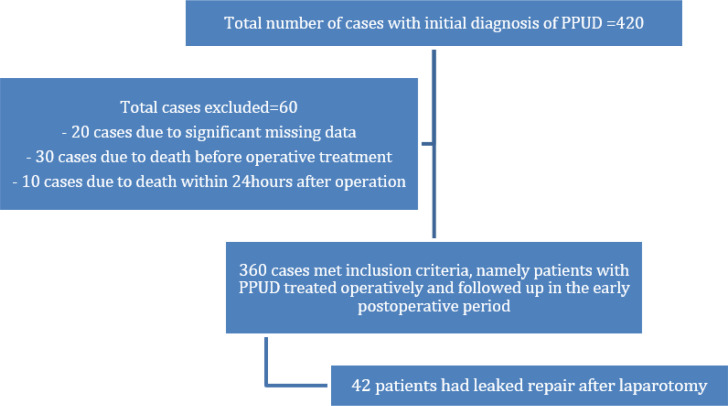
Methods: This is a multicenter cross-sectional study of leaked repair after omental patch of PPUD between January 2016 to December 2022. Following primary repair of PPUD with omental pedicle reinforcement, associated factors of leaked repair were evaluated using univariate and multivariate analyses.
Results: Overall, 360 cases were evaluated (62.8% male). Leaked repair rate was 11.7% (42 cases). Those without immunosuppression were 3 times less likely to have leaked repair (aOR= 0.34; 95% CI: 0.16 - 0.72; p = 0.003) while those with sepsis were 4 times more likely to have leaked repair (aOR=4.16; 95% CI: 1.06 - 12.36; p = 0.018). Patients with delayed presentation (>48 hours) were 2.5 times more likely to have leaked repair than those who presented in 0 - 24 hours (aOR=2.51; 95% CI: 3.62 - 10.57; p = 0.044). Those with Perforation diameter 2.1-3.0 cm were 8 times (aOR=7.98; 95% CI: 2.63-24.21; p<0.0001), and those with perforation diameter > 3.0cm were 33 times (aOR=33.04; 95% CI: 10.98-100.25; p<0.0001) more likely to have leaked repair than those with perforation diameter of 0-1.0 cm. Similarly, in those with no perioperative shock, leaked repair was 4 times less likely to develop than those with perioperative shock (aOR= 0.42; 95% CI: 0.41-0.92; p = 0.041). There was significant statistical difference in morbidity (p = 0.003) and mortality (p < 0.0001) rates for cases of leaked repairs and successful repairs.
Conclusion: Leaked repair following omentopexy for peptic ulcer perforation was significantly associated with large perforation diameter, delayed presentation, sepsis, immunosuppressive therapy, and perioperative shock.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
