Clara Oliveira, Beatrice Mainoli, Gonçalo S Duarte, Tiago Machado, Rita G Tinoco, Miguel Esperança-Martins, Joaquim J Ferreira, João Costa
{"title":"Immune-related serious adverse events with immune checkpoint inhibitors: Systematic review and network meta-analysis.","authors":"Clara Oliveira, Beatrice Mainoli, Gonçalo S Duarte, Tiago Machado, Rita G Tinoco, Miguel Esperança-Martins, Joaquim J Ferreira, João Costa","doi":"10.1007/s00228-024-03647-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Immune checkpoint inhibitors (ICIs) have revolutionized cancer treatment, though uncertainty exists regarding their immune-related safety. The objective of this study was to assess the comparative safety profile (odds ratio) of ICIs and estimate the absolute rate of immune-related serious adverse events (irSAEs) in cancer patients undergoing treatment with ICIs.</p><p><strong>Methods: </strong>We searched for randomized trials till February 2021, including all ICIs for all cancers. Primary outcome was overall irSAEs, and secondary outcomes were pneumonitis, colitis, hepatitis, hypophysitis, myocarditis, nephritis, and pancreatitis. We conducted Bayesian network meta-analyses, estimated absolute rates and ranked treatments according to the surface under the cumulative ranking curve (SUCRA).</p><p><strong>Results: </strong>We included 96 trials (52,811 participants, median age 62 years). Risk of bias was high in most trials. Most cancers were non-small cell lung cancer (28 trials) and melanoma (15 trials). The worst-ranked ICI was ipilimumab (SUCRA 14%; event rate 848/10,000 patients) while the best-ranked ICI was atezolizumab (SUCRA 82%; event rate 119/10,000 patients).</p><p><strong>Conclusion: </strong>Each ICI showed a unique safety profile, with certain events more frequently observed with specific ICIs, which should be considered when managing cancer patients.</p>","PeriodicalId":11857,"journal":{"name":"European Journal of Clinical Pharmacology","volume":" ","pages":"677-684"},"PeriodicalIF":2.7000,"publicationDate":"2024-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11001692/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Clinical Pharmacology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00228-024-03647-z","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/19 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Immune checkpoint inhibitors (ICIs) have revolutionized cancer treatment, though uncertainty exists regarding their immune-related safety. The objective of this study was to assess the comparative safety profile (odds ratio) of ICIs and estimate the absolute rate of immune-related serious adverse events (irSAEs) in cancer patients undergoing treatment with ICIs.
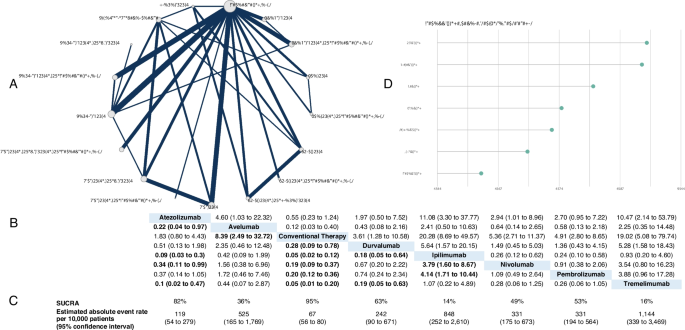
Methods: We searched for randomized trials till February 2021, including all ICIs for all cancers. Primary outcome was overall irSAEs, and secondary outcomes were pneumonitis, colitis, hepatitis, hypophysitis, myocarditis, nephritis, and pancreatitis. We conducted Bayesian network meta-analyses, estimated absolute rates and ranked treatments according to the surface under the cumulative ranking curve (SUCRA).
Results: We included 96 trials (52,811 participants, median age 62 years). Risk of bias was high in most trials. Most cancers were non-small cell lung cancer (28 trials) and melanoma (15 trials). The worst-ranked ICI was ipilimumab (SUCRA 14%; event rate 848/10,000 patients) while the best-ranked ICI was atezolizumab (SUCRA 82%; event rate 119/10,000 patients).
Conclusion: Each ICI showed a unique safety profile, with certain events more frequently observed with specific ICIs, which should be considered when managing cancer patients.
期刊介绍:
The European Journal of Clinical Pharmacology publishes original papers on all aspects of clinical pharmacology and drug therapy in humans. Manuscripts are welcomed on the following topics: therapeutic trials, pharmacokinetics/pharmacodynamics, pharmacogenetics, drug metabolism, adverse drug reactions, drug interactions, all aspects of drug development, development relating to teaching in clinical pharmacology, pharmacoepidemiology, and matters relating to the rational prescribing and safe use of drugs. Methodological contributions relevant to these topics are also welcomed.
Data from animal experiments are accepted only in the context of original data in man reported in the same paper. EJCP will only consider manuscripts describing the frequency of allelic variants in different populations if this information is linked to functional data or new interesting variants. Highly relevant differences in frequency with a major impact in drug therapy for the respective population may be submitted as a letter to the editor.
Straightforward phase I pharmacokinetic or pharmacodynamic studies as parts of new drug development will only be considered for publication if the paper involves
-a compound that is interesting and new in some basic or fundamental way, or
-methods that are original in some basic sense, or
-a highly unexpected outcome, or
-conclusions that are scientifically novel in some basic or fundamental sense.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
