{"title":"Prognostic Analysis of Stage I Non-Small Cell Lung Cancer Abutting Adjacent Structures on Preoperative Computed Tomography.","authors":"Soohwan Choi, Sun Kyun Ro, Seok Whan Moon","doi":"10.5090/jcs.23.153","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Early non-small cell lung cancer (NSCLC) that abuts adjacent structures requires careful evaluation due to its potential impact on postoperative outcomes and prognosis. We examined stage I NSCLC with invasion into adjacent structures, focusing on the prognostic implications after curative surgical resection.</p><p><strong>Methods: </strong>We retrospectively analyzed the records of 796 patients who underwent curative surgical resection for pathologic stage IA/IB NSCLC (i.e., visceral pleural invasion only) at a single center from 2008 to 2017. Patients were classified based on tumor abutment and then reclassified by the presence of visceral pleural invasion. Clinical characteristics, pathological features, and survival rates were compared.</p><p><strong>Results: </strong>The study included 181 patients with abutting NSCLC (22.7% of all participants) and 615 with non-abutting tumors (77.3%). Those with tumor abutment exhibited higher rates of non-adenocarcinoma (26.5% vs. 9.9%, p<0.01) and visceral/lymphatic/vascular invasion (30.4%/33.1%/12.7% vs. 8.5%/22.4%/5.7%, respectively; p<0.01) compared to those without abutment. Multivariable analysis identified lymphatic invasion and male sex as risk factors for overall survival (OS) and disease-free survival (DFS) in stage I NSCLC measuring 3 cm or smaller. Age, smoking history, vascular invasion, and recurrence emerged as risk factors for OS, whereas the presence of non-pure ground-glass opacity was a risk factor for DFS.</p><p><strong>Conclusion: </strong>NSCLC lesions 3 cm or smaller that abut adjacent structures present higher rates of various risk factors than non-abutting lesions, necessitating evaluation of tumor invasion into adjacent structures and lymph node metastasis. In isolation, however, the presence of tumor abutment without visceral pleural invasion does not constitute a risk factor.</p>","PeriodicalId":34499,"journal":{"name":"Journal of Chest Surgery","volume":" ","pages":"136-144"},"PeriodicalIF":1.0000,"publicationDate":"2024-03-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10927430/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Chest Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5090/jcs.23.153","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/20 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Early non-small cell lung cancer (NSCLC) that abuts adjacent structures requires careful evaluation due to its potential impact on postoperative outcomes and prognosis. We examined stage I NSCLC with invasion into adjacent structures, focusing on the prognostic implications after curative surgical resection.
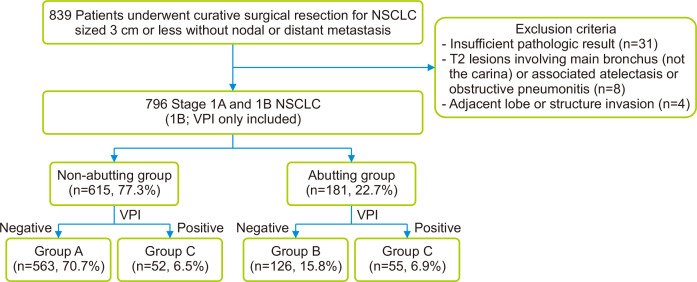
Methods: We retrospectively analyzed the records of 796 patients who underwent curative surgical resection for pathologic stage IA/IB NSCLC (i.e., visceral pleural invasion only) at a single center from 2008 to 2017. Patients were classified based on tumor abutment and then reclassified by the presence of visceral pleural invasion. Clinical characteristics, pathological features, and survival rates were compared.
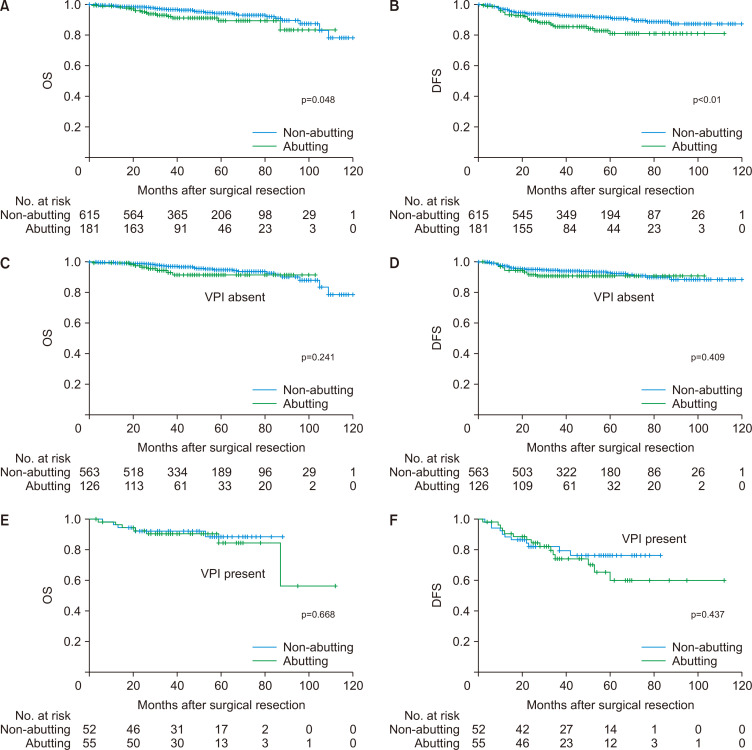
Results: The study included 181 patients with abutting NSCLC (22.7% of all participants) and 615 with non-abutting tumors (77.3%). Those with tumor abutment exhibited higher rates of non-adenocarcinoma (26.5% vs. 9.9%, p<0.01) and visceral/lymphatic/vascular invasion (30.4%/33.1%/12.7% vs. 8.5%/22.4%/5.7%, respectively; p<0.01) compared to those without abutment. Multivariable analysis identified lymphatic invasion and male sex as risk factors for overall survival (OS) and disease-free survival (DFS) in stage I NSCLC measuring 3 cm or smaller. Age, smoking history, vascular invasion, and recurrence emerged as risk factors for OS, whereas the presence of non-pure ground-glass opacity was a risk factor for DFS.
Conclusion: NSCLC lesions 3 cm or smaller that abut adjacent structures present higher rates of various risk factors than non-abutting lesions, necessitating evaluation of tumor invasion into adjacent structures and lymph node metastasis. In isolation, however, the presence of tumor abutment without visceral pleural invasion does not constitute a risk factor.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
