{"title":"The role of Point-of-Care Ultrasound of pupil for pupillometry in subarachnoid hemorrhage","authors":"Priyanka Modi, Sanjeev Bhoi, Pallavi Sinha, Savan Pandey","doi":"10.1002/ird3.52","DOIUrl":null,"url":null,"abstract":"<p>A 60-year-old woman presented to the emergency department, previously diagnosed in other hospital with acute subarachnoid hemorrhage (SAH) involving left proximal Sylvian and anterior interhemispheric sinuses. On presentation, her airway was patent, pulse rate was 86 beats per minute, blood pressure was 112/76 mmHg, respiratory rate was 18 beats per minute, SpO<sub>2</sub> was 99% on room air, Glasgow Coma Score was 11 (E3V3M5), and pupils were bilaterally (B/L) mid-dilated, reactive to light, and afebrile to touch. Neurological examination was limited due to altered sensorium: No neck rigidity; sensory functions, all cranial nerves, and cerebellar signs were not assessed; motor examination: power could not be assessed; B/L upper and lower limbs tone were decreased; B/L upper and lower limbs reflexes were normal; and B/L Plantar flexion were present. Her laboratory parameters were sodium 146.4 mmol/L, potassium 4.53 mmol/L, chloride 119.3 mmol/L, total bilirubin 55.23 μmol/L, creatinine 90.17 μmol/L, urea 8391.61 μmol/L, and INR 1.127.</p><p>A linear probe (frequency of 7–12 MHz) of Point-of-Care Ultrasound (POCUS) systems was utilized for pupillometry. There was anisocoria of 0.7 mm (the size of right and left pupils were 4.2 and 3.5 mm, respectively, Figure 1a,b). The bilateral pupil during direct light stimulation revealed briskly reactive pupils with rebound dilatation (Video 1a,b). However, the bilateral pupil during consensual light stimulation revealed a normal reactive pupil with no rebound dilatation (Video 1c,d). The patient was managed conservatively and referred to another hospital. She had decompression craniectomy on further deterioration of GCS. She died after 1 month due to infective complications of surgery.</p><p>Intracranial pressure can be raised due to any supratentorial mass lesion or head trauma. A common problem in the emergency department is how to decide when operative decompression is urgently required in them. Although computed tomography scans are standard tests for definitive diagnosis of brain stem compression, it is inconvenient to use to monitor for the requirement of surgical intervention. In addition, a more precise assessment of the pupil by manual examination is problematic due to large inter-examiner variability. Hence, there are no specific manual pupillary assessment findings for diagnosing brain stem compression. Some clinicians suggest that infrared pupillary scan findings, such as anisocoria of greater than 3 mm and reduced light reflexes, are predictive of an expanding mass lesion in the brain [<span>1</span>]. However, portable infrared pupillometers are not widely available. On the other hand, POCUS, a simple, objective, and quick imaging tool with an additional advantage of recording, is increasingly available for emergency imaging needs [<span>2</span>].</p><p>The raised intracranial pressure, sequelae of acute nontraumatic SAH, may cause compressive optic neuropathy and papilledema. Complications of compressive optic neuropathy and papilledema can cause relative afferent pupillary defect (RAPD), etc. Also, cerebral vasospasm following acute nontraumatic SAH, a severe complication, occurs in about 75% of patients surviving initial bleeding and leads to delayed cerebral ischemia in 17%–40% of patients. Ischemic optic neuropathy (ION), which is the result of vascular insufficiency in the optic nerve, is seen in SAH [<span>3, 4</span>]. An RAPD (with paradoxical pupillary dilatation in response to light) is an important sign of optic nerve disease or injury. If present, it confirms the lesion like ION in the pupil pathway on the afferent side. During POCUS study, this RAPD may be seen as an abnormal direct pupillary light reflex in the form of rebound dilatation or hippus and normal contralateral pupillary light reflex prior to the development of any clinically significant loss of vision. Rebound dilation (previously known as pupillary unrest) is defined as “a period of constriction followed by dilation with a change equal to or greater than 2 mm.” Hippus is defined as a “rhythmic pulsation of the pupils of the eyes, as they dilate and constrict within fixed limits” [<span>5</span>]. However, future studies are required to validate this observation.</p><p>Priyanka Modi analyzed the data and prepared the first draft of the manuscript. Priyanka Modi, Sanjeev Bhoi, Pallavi Sinha, and Savan Pandey participated in the conception and design of the study; Priyanka Modi constructively revised the manuscript, participated in data collection and organization, participated in and supervised the study throughout. All authors commented on previous versions of the manuscript and approved the final version.</p><p>The authors declare no conflicts of interest.</p><p>Not applicable.</p><p>The patient provided written informed consent at the time of entering this study.</p>","PeriodicalId":73508,"journal":{"name":"iRadiology","volume":"2 1","pages":"99-101"},"PeriodicalIF":0.0000,"publicationDate":"2024-01-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ird3.52","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"iRadiology","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ird3.52","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
A 60-year-old woman presented to the emergency department, previously diagnosed in other hospital with acute subarachnoid hemorrhage (SAH) involving left proximal Sylvian and anterior interhemispheric sinuses. On presentation, her airway was patent, pulse rate was 86 beats per minute, blood pressure was 112/76 mmHg, respiratory rate was 18 beats per minute, SpO2 was 99% on room air, Glasgow Coma Score was 11 (E3V3M5), and pupils were bilaterally (B/L) mid-dilated, reactive to light, and afebrile to touch. Neurological examination was limited due to altered sensorium: No neck rigidity; sensory functions, all cranial nerves, and cerebellar signs were not assessed; motor examination: power could not be assessed; B/L upper and lower limbs tone were decreased; B/L upper and lower limbs reflexes were normal; and B/L Plantar flexion were present. Her laboratory parameters were sodium 146.4 mmol/L, potassium 4.53 mmol/L, chloride 119.3 mmol/L, total bilirubin 55.23 μmol/L, creatinine 90.17 μmol/L, urea 8391.61 μmol/L, and INR 1.127.
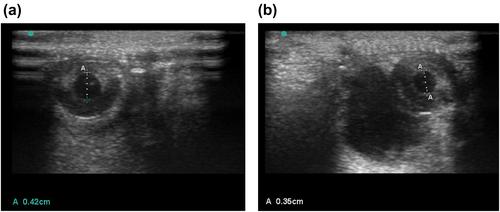
A linear probe (frequency of 7–12 MHz) of Point-of-Care Ultrasound (POCUS) systems was utilized for pupillometry. There was anisocoria of 0.7 mm (the size of right and left pupils were 4.2 and 3.5 mm, respectively, Figure 1a,b). The bilateral pupil during direct light stimulation revealed briskly reactive pupils with rebound dilatation (Video 1a,b). However, the bilateral pupil during consensual light stimulation revealed a normal reactive pupil with no rebound dilatation (Video 1c,d). The patient was managed conservatively and referred to another hospital. She had decompression craniectomy on further deterioration of GCS. She died after 1 month due to infective complications of surgery.
Intracranial pressure can be raised due to any supratentorial mass lesion or head trauma. A common problem in the emergency department is how to decide when operative decompression is urgently required in them. Although computed tomography scans are standard tests for definitive diagnosis of brain stem compression, it is inconvenient to use to monitor for the requirement of surgical intervention. In addition, a more precise assessment of the pupil by manual examination is problematic due to large inter-examiner variability. Hence, there are no specific manual pupillary assessment findings for diagnosing brain stem compression. Some clinicians suggest that infrared pupillary scan findings, such as anisocoria of greater than 3 mm and reduced light reflexes, are predictive of an expanding mass lesion in the brain [1]. However, portable infrared pupillometers are not widely available. On the other hand, POCUS, a simple, objective, and quick imaging tool with an additional advantage of recording, is increasingly available for emergency imaging needs [2].
The raised intracranial pressure, sequelae of acute nontraumatic SAH, may cause compressive optic neuropathy and papilledema. Complications of compressive optic neuropathy and papilledema can cause relative afferent pupillary defect (RAPD), etc. Also, cerebral vasospasm following acute nontraumatic SAH, a severe complication, occurs in about 75% of patients surviving initial bleeding and leads to delayed cerebral ischemia in 17%–40% of patients. Ischemic optic neuropathy (ION), which is the result of vascular insufficiency in the optic nerve, is seen in SAH [3, 4]. An RAPD (with paradoxical pupillary dilatation in response to light) is an important sign of optic nerve disease or injury. If present, it confirms the lesion like ION in the pupil pathway on the afferent side. During POCUS study, this RAPD may be seen as an abnormal direct pupillary light reflex in the form of rebound dilatation or hippus and normal contralateral pupillary light reflex prior to the development of any clinically significant loss of vision. Rebound dilation (previously known as pupillary unrest) is defined as “a period of constriction followed by dilation with a change equal to or greater than 2 mm.” Hippus is defined as a “rhythmic pulsation of the pupils of the eyes, as they dilate and constrict within fixed limits” [5]. However, future studies are required to validate this observation.
Priyanka Modi analyzed the data and prepared the first draft of the manuscript. Priyanka Modi, Sanjeev Bhoi, Pallavi Sinha, and Savan Pandey participated in the conception and design of the study; Priyanka Modi constructively revised the manuscript, participated in data collection and organization, participated in and supervised the study throughout. All authors commented on previous versions of the manuscript and approved the final version.
The authors declare no conflicts of interest.
Not applicable.
The patient provided written informed consent at the time of entering this study.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
