Effect of ferric citrate hydrate on fibroblast growth factor 23 and platelets in non-dialysis-dependent chronic kidney disease and non-chronic kidney disease patients with iron deficiency anemia.
{"title":"Effect of ferric citrate hydrate on fibroblast growth factor 23 and platelets in non-dialysis-dependent chronic kidney disease and non-chronic kidney disease patients with iron deficiency anemia.","authors":"Kyoko Ito, Tadao Akizawa, Kojo Arita, Yuko Mitobe, Norio Komatsu","doi":"10.1007/s10157-023-02455-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Iron deficiency anemia (IDA) increases levels of C-terminal fibroblast growth factor 23 (cFGF23) and platelet count (PLT), each of which is associated with cardiovascular events. Therefore, we hypothesized that iron replacement with ferric citrate hydrate (FC) would decrease cFGF23 levels and PLT in patients with IDA.</p><p><strong>Methods: </strong>In a randomized, open-label, multicenter, 24-week clinical trial, patients with non-dialysis-dependent chronic kidney disease (CKD) and non-CKD complicated by IDA (8.0 ≤ hemoglobin < 11.0 g/dL; and serum ferritin < 50 ng/mL [CKD]; < 12 ng/mL [non-CKD]) were randomized 1:1 to FC-low (500 mg: approximately 120 mg elemental iron/day) or FC-high (1000 mg: approximately 240 mg elemental iron/day). If sufficient iron replacement had been achieved after week 8, further treatment was discontinued.</p><p><strong>Results: </strong>Seventy-three patients were allocated to FC-low (CKD n = 21, non-CKD n = 15) and FC-high (CKD n = 21, non-CKD n = 16). Regardless of CKD status, FC increased serum ferritin and transferrin saturation, did not change intact FGF23 or serum phosphorus, but decreased cFGF23. In FC-low group, median changes in cFGF23 from baseline to week 8 were -58.00 RU/mL in CKD and -725.00 RU/mL in non-CKD; in FC-high group, the median changes were -66.00 RU/mL in CKD and -649.50 RU/mL in non-CKD. By week 8, FC treatment normalized PLT in all patients with high PLT at baseline (>35.2 × 10<sup>4</sup>/µL; FC-low: 1 CKD, 8 non-CKD; FC-high: 3 CKD, 8 non-CKD).</p><p><strong>Conclusion: </strong>Regardless of CKD status, iron replacement with FC decreased elevated cFGF23 levels and normalized elevated PLT in patients with IDA.</p><p><strong>Clinical trial registration number: </strong>jRCT2080223943.</p>","PeriodicalId":10349,"journal":{"name":"Clinical and Experimental Nephrology","volume":" ","pages":"636-646"},"PeriodicalIF":1.7000,"publicationDate":"2024-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11189996/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Nephrology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10157-023-02455-6","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/25 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Iron deficiency anemia (IDA) increases levels of C-terminal fibroblast growth factor 23 (cFGF23) and platelet count (PLT), each of which is associated with cardiovascular events. Therefore, we hypothesized that iron replacement with ferric citrate hydrate (FC) would decrease cFGF23 levels and PLT in patients with IDA.
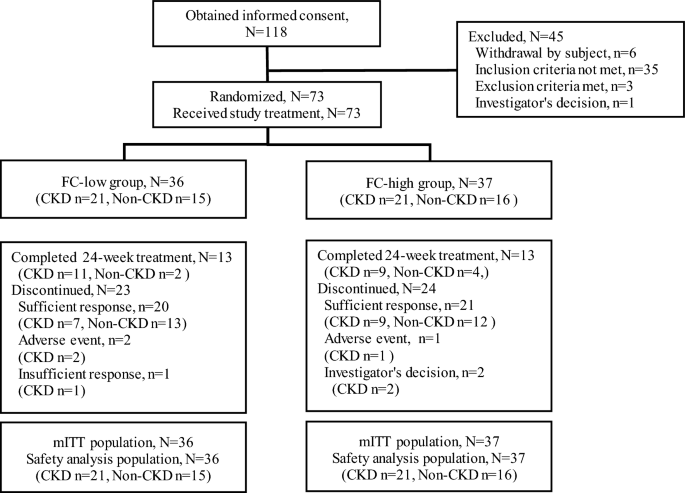
Methods: In a randomized, open-label, multicenter, 24-week clinical trial, patients with non-dialysis-dependent chronic kidney disease (CKD) and non-CKD complicated by IDA (8.0 ≤ hemoglobin < 11.0 g/dL; and serum ferritin < 50 ng/mL [CKD]; < 12 ng/mL [non-CKD]) were randomized 1:1 to FC-low (500 mg: approximately 120 mg elemental iron/day) or FC-high (1000 mg: approximately 240 mg elemental iron/day). If sufficient iron replacement had been achieved after week 8, further treatment was discontinued.
Results: Seventy-three patients were allocated to FC-low (CKD n = 21, non-CKD n = 15) and FC-high (CKD n = 21, non-CKD n = 16). Regardless of CKD status, FC increased serum ferritin and transferrin saturation, did not change intact FGF23 or serum phosphorus, but decreased cFGF23. In FC-low group, median changes in cFGF23 from baseline to week 8 were -58.00 RU/mL in CKD and -725.00 RU/mL in non-CKD; in FC-high group, the median changes were -66.00 RU/mL in CKD and -649.50 RU/mL in non-CKD. By week 8, FC treatment normalized PLT in all patients with high PLT at baseline (>35.2 × 104/µL; FC-low: 1 CKD, 8 non-CKD; FC-high: 3 CKD, 8 non-CKD).
Conclusion: Regardless of CKD status, iron replacement with FC decreased elevated cFGF23 levels and normalized elevated PLT in patients with IDA.
期刊介绍:
Clinical and Experimental Nephrology is a peer-reviewed monthly journal, officially published by the Japanese Society of Nephrology (JSN) to provide an international forum for the discussion of research and issues relating to the study of nephrology. Out of respect for the founders of the JSN, the title of this journal uses the term “nephrology,” a word created and brought into use with the establishment of the JSN (Japanese Journal of Nephrology, Vol. 2, No. 1, 1960). The journal publishes articles on all aspects of nephrology, including basic, experimental, and clinical research, so as to share the latest research findings and ideas not only with members of the JSN, but with all researchers who wish to contribute to a better understanding of recent advances in nephrology. The journal is unique in that it introduces to an international readership original reports from Japan and also the clinical standards discussed and agreed by JSN.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
