Demonstrating Bioequivalence for Two Dose Strengths of Niraparib and Abiraterone Acetate Dual-Action Tablets Versus Single Agents: Utility of Clinical Study Data Supplemented with Modeling and Simulation.
Alex Yu, Anasuya Hazra, James Juhui Jiao, Peter Hellemans, Anna Mitselos, Hui Tian, Juan Jose Perez Ruixo, Nahor Haddish-Berhane, Daniele Ouellet, Alberto Russu
{"title":"Demonstrating Bioequivalence for Two Dose Strengths of Niraparib and Abiraterone Acetate Dual-Action Tablets Versus Single Agents: Utility of Clinical Study Data Supplemented with Modeling and Simulation.","authors":"Alex Yu, Anasuya Hazra, James Juhui Jiao, Peter Hellemans, Anna Mitselos, Hui Tian, Juan Jose Perez Ruixo, Nahor Haddish-Berhane, Daniele Ouellet, Alberto Russu","doi":"10.1007/s40262-023-01340-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objective: </strong>The combination of niraparib and abiraterone acetate (AA) plus prednisone is under investigation for the treatment of patients with metastatic castration-resistant prostate cancer (mCRPC) and metastatic castration-sensitive prostate cancer (mCSPC). Regular-strength (RS) and lower-strength (LS) dual-action tablets (DATs), comprising niraparib 100 mg/AA 500 mg and niraparib 50 mg/AA 500 mg, respectively, were developed to reduce pill burden and improve patient experience. A bioequivalence (BE)/bioavailability (BA) study was conducted under modified fasting conditions in patients with mCRPC to support approval of the DATs.</p><p><strong>Methods: </strong>This open-label randomized BA/BE study (NCT04577833) was conducted at 14 sites in the USA and Europe. The study had a sequential design, including a 21-day screening phase, a pharmacokinetic (PK) assessment phase comprising three periods [namely (1) single-dose with up to 1-week run-in, (2) daily dose on days 1-11, and (3) daily dose on days 12-22], an extension where both niraparib and AA as single-agent combination (SAC; reference) or AA alone was continued from day 23 until discontinuation, and a 30-day follow-up phase. Patients were randomly assigned in a parallel-group design (four-sequence randomization) to receive a single oral dose of niraparib 100 mg/AA 1000 mg as a LS-DAT or SAC in period 1, and patients continued as randomized into a two-way crossover design during periods 2 and 3 where they received niraparib 200 mg/AA 1000 mg once daily as a RS-DAT or SAC. The design was powered on the basis of crossover assessment of RS-DAT versus SAC. During repeated dosing (periods 2 and 3, and extension phase), all patients also received prednisone/prednisolone 5 mg twice daily. Plasma samples were collected for measurement of niraparib and abiraterone plasma concentrations. Statistical assessment of the RS-DAT and LS-DAT versus SAC was performed on log-transformed pharmacokinetic parameters data from periods 2 and 3 (crossover) and from period 1 (parallel), respectively. Additional paired analyses and model-based bioequivalence assessments were conducted to evaluate the similarity between the LS-DAT and SAC.</p><p><strong>Results: </strong>For the RS-DAT versus SAC, the 90% confidence intervals (CI) of geometric mean ratios (GMR) for maximum concentration at a steady state (C<sub>max,ss</sub>) and area under the plasma concentration-time curve from 0-24 h at a steady state (AUC <sub>0-24h,ss</sub>) were respectively 99.18-106.12% and 97.91-104.31% for niraparib and 87.59-106.69 and 86.91-100.23% for abiraterone. For the LS-DAT vs SAC, the 90% CI of GMR for AUC<sub>0-72h</sub> of niraparib was 80.31-101.12% in primary analysis, the 90% CI of GMR for C<sub>max,ss</sub> and AUC <sub>0-24h</sub>,ss of abiraterone was 85.41-118.34% and 86.51-121.64% respectively, and 96.4% of simulated LS-DAT versus SAC BE trials met the BE criteria for both niraparib and abiraterone.</p><p><strong>Conclusions: </strong>The RS-DAT met BE criteria (range 80%-125%) versus SAC based on 90% CI of GMR for C<sub>max,ss</sub> and AUC <sub>0-24h,ss</sub>. The LS-DAT was considered BE to SAC on the basis of the niraparib component meeting the BE criteria in the primary analysis for AUC <sub>0-72h</sub>; abiraterone meeting the BE criteria in additional paired analyses based on C<sub>max,ss</sub> and AUC <sub>0-24h,ss</sub>; and the percentage of simulated LS-DAT versus SAC BE trials meeting the BE criteria for both.</p><p><strong>Clinicaltrials: </strong></p><p><strong>Gov identifier: </strong>NCT04577833.</p>","PeriodicalId":10405,"journal":{"name":"Clinical Pharmacokinetics","volume":" ","pages":"511-527"},"PeriodicalIF":4.0000,"publicationDate":"2024-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11052869/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Pharmacokinetics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40262-023-01340-5","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/4 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and objective: The combination of niraparib and abiraterone acetate (AA) plus prednisone is under investigation for the treatment of patients with metastatic castration-resistant prostate cancer (mCRPC) and metastatic castration-sensitive prostate cancer (mCSPC). Regular-strength (RS) and lower-strength (LS) dual-action tablets (DATs), comprising niraparib 100 mg/AA 500 mg and niraparib 50 mg/AA 500 mg, respectively, were developed to reduce pill burden and improve patient experience. A bioequivalence (BE)/bioavailability (BA) study was conducted under modified fasting conditions in patients with mCRPC to support approval of the DATs.
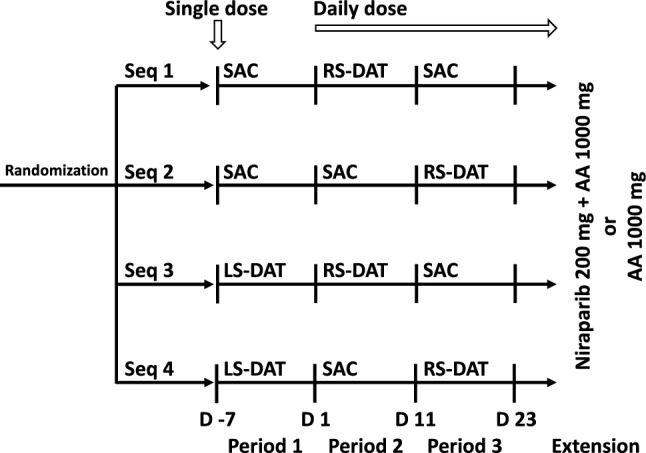
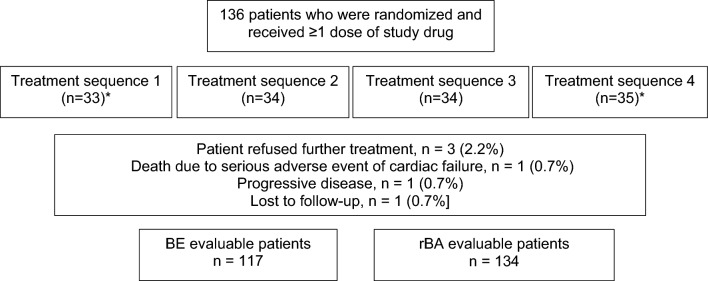
Methods: This open-label randomized BA/BE study (NCT04577833) was conducted at 14 sites in the USA and Europe. The study had a sequential design, including a 21-day screening phase, a pharmacokinetic (PK) assessment phase comprising three periods [namely (1) single-dose with up to 1-week run-in, (2) daily dose on days 1-11, and (3) daily dose on days 12-22], an extension where both niraparib and AA as single-agent combination (SAC; reference) or AA alone was continued from day 23 until discontinuation, and a 30-day follow-up phase. Patients were randomly assigned in a parallel-group design (four-sequence randomization) to receive a single oral dose of niraparib 100 mg/AA 1000 mg as a LS-DAT or SAC in period 1, and patients continued as randomized into a two-way crossover design during periods 2 and 3 where they received niraparib 200 mg/AA 1000 mg once daily as a RS-DAT or SAC. The design was powered on the basis of crossover assessment of RS-DAT versus SAC. During repeated dosing (periods 2 and 3, and extension phase), all patients also received prednisone/prednisolone 5 mg twice daily. Plasma samples were collected for measurement of niraparib and abiraterone plasma concentrations. Statistical assessment of the RS-DAT and LS-DAT versus SAC was performed on log-transformed pharmacokinetic parameters data from periods 2 and 3 (crossover) and from period 1 (parallel), respectively. Additional paired analyses and model-based bioequivalence assessments were conducted to evaluate the similarity between the LS-DAT and SAC.
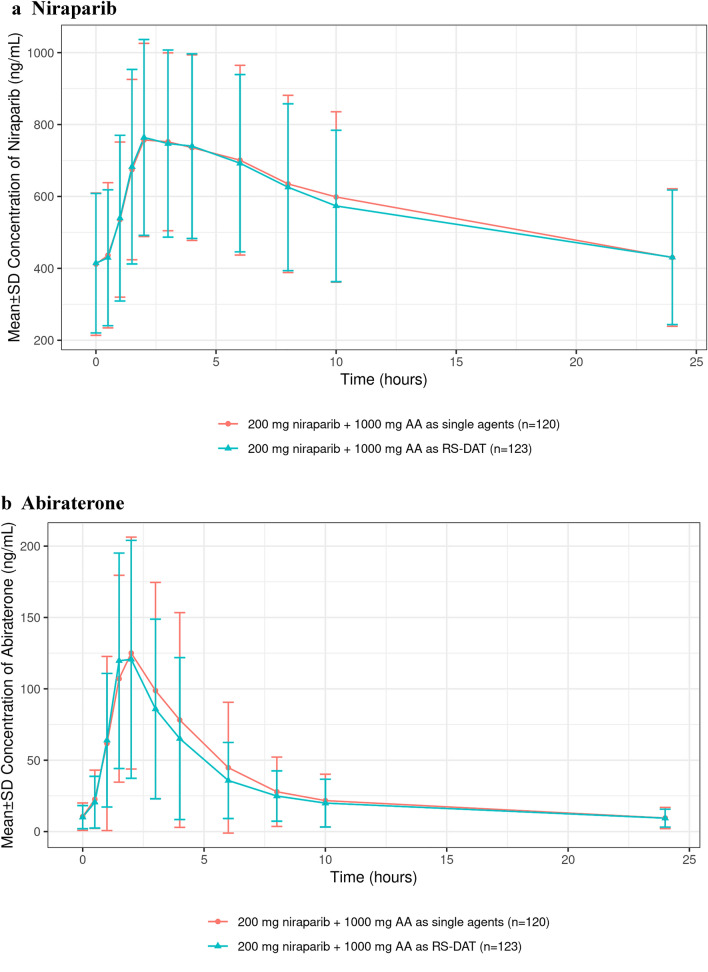
Results: For the RS-DAT versus SAC, the 90% confidence intervals (CI) of geometric mean ratios (GMR) for maximum concentration at a steady state (Cmax,ss) and area under the plasma concentration-time curve from 0-24 h at a steady state (AUC 0-24h,ss) were respectively 99.18-106.12% and 97.91-104.31% for niraparib and 87.59-106.69 and 86.91-100.23% for abiraterone. For the LS-DAT vs SAC, the 90% CI of GMR for AUC0-72h of niraparib was 80.31-101.12% in primary analysis, the 90% CI of GMR for Cmax,ss and AUC 0-24h,ss of abiraterone was 85.41-118.34% and 86.51-121.64% respectively, and 96.4% of simulated LS-DAT versus SAC BE trials met the BE criteria for both niraparib and abiraterone.
Conclusions: The RS-DAT met BE criteria (range 80%-125%) versus SAC based on 90% CI of GMR for Cmax,ss and AUC 0-24h,ss. The LS-DAT was considered BE to SAC on the basis of the niraparib component meeting the BE criteria in the primary analysis for AUC 0-72h; abiraterone meeting the BE criteria in additional paired analyses based on Cmax,ss and AUC 0-24h,ss; and the percentage of simulated LS-DAT versus SAC BE trials meeting the BE criteria for both.
期刊介绍:
Clinical Pharmacokinetics promotes the continuing development of clinical pharmacokinetics and pharmacodynamics for the improvement of drug therapy, and for furthering postgraduate education in clinical pharmacology and therapeutics.
Pharmacokinetics, the study of drug disposition in the body, is an integral part of drug development and rational use. Knowledge and application of pharmacokinetic principles leads to accelerated drug development, cost effective drug use and a reduced frequency of adverse effects and drug interactions.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
