{"title":"Revealing the secret behind Epstein-Barr virus-specific tumor immune contexture","authors":"Chu-Xia Deng","doi":"10.1002/cac2.12529","DOIUrl":null,"url":null,"abstract":"<p>Immune checkpoint inhibitor (ICI) therapy has significantly revolutionized cancer treatment across various malignancies, offering distinct and enduring clinical advantages [<span>1</span>]. Gastric cancer (GC) represents a widespread and life-threatening malignancy with substantial global health implications [<span>2</span>]. However, ICI therapy has not produced satisfactory therapeutic responses in GC patients. Presently, monotherapy targeting the programmed cell death protein 1/programmed death-ligand 1 (PD-1/PD-L1) pathway demonstrates clinical efficacy in approximately 10% of GC patients [<span>3</span>]. Exploration of novel immunotherapeutic targets is urgently needed. Notably, Epstein-Barr virus (EBV)-positive GC constitutes a distinct GC subset, exhibiting a remarkably higher objective response rate to anti-PD-1 inhibitors—an intriguing phenomenon [<span>4</span>]. Several studies have found that EBV-positive GC has more innate and adaptive immune cell infiltration than EBV-negative GC [<span>5, 6</span>]. In their recent publication titled “Dynamic single-cell mapping reveals Epstein-Barr virus-imprinted T-cell exhaustion and on-treatment response”, Qiu <i>et al.</i> [<span>7</span>] unveiled, for the first time, the cellular basis underlying these remarkably heightened responses in EBV-positive GC patients undergoing immunochemotherapy. Leveraging single-cell profiling technologies, this study deepened our comprehension of the intricate and heterogeneous tumor microenvironment in GC.</p><p>In this study, the authors conducted a comprehensive characterization of the cellular dynamics of tumor-infiltrating immune cells in GC patients, distinguishing between those with EBV-positive and EBV-negative statuses. EBV-positive GC exhibited a heightened immune phenotype characterized by elevated infiltration of T cells and B cells, highlighting the intricate interplay among EBV infection, multi-cellular ecosystems, and tumor development. EBV-negative GC exhibited an immune-suppressive tumor microenvironment characterized by an abundance of plasma cells, myeloid cells, and mast cells. After treatment, the evaluation of the dynamic changes in EBV-positive GC showed an increased presence of cytotoxic CD8<sup>+</sup> T cells and effector memory/memory CD8<sup>+</sup> T cells. Notably, there was clear evidence of clonal revival and reinvigoration of CD8<sup>+</sup> T cells in EBV-positive GC patients, indicating an active T cell-mediated immune reaction enhancing treatment responses.</p><p>Furthermore, the authors observed a distinct EBV-imprinted CD8<sup>+</sup> T cell population, ISG-15<sup>+</sup>CD8<sup>+</sup> T cells, which exhibited significantly higher expression of interferon-stimulated genes, such as ISG-15, IFIT1-3, RASD2, and MX1. Significantly, ISG-15<sup>+</sup>CD8<sup>+</sup> T cells demonstrated the ability to recognize EBV antigens and coordinated exhausted T cell responses. STARTRAC-tran analysis revealed a robust association between ISG-15<sup>+</sup>CD8<sup>+</sup> T cells and actively proliferating T cells, effector CD8<sup>+</sup> T cells (CXCL13<sup>+</sup>CD8<sup>+</sup> T cells) and cytotoxic CD8<sup>+</sup> T cells within EBV-positive GC. It is worth mentioning that EBV epitopes were detected within ISG-15<sup>+</sup>CD8<sup>+</sup> T cells, suggesting that this particular cell population consists of T cells specifically targeting EBV. In the context of ICI-responsive GCs, their investigation revealed a significant proportion of ISG-15<sup>+</sup>CD8<sup>+</sup> T clonotypes prior to treatment within the effector T cell populations of EBV-positive tumors after the treatment. In contrast, there was no evidence of re-emerged clonotypes of pre-existing ISG-15<sup>+</sup>CD8<sup>+</sup> T cells in EBV-negative tumors following therapy. More research is required to validate these observations, as these data suggest that ISG-15<sup>+</sup>CD8<sup>+</sup> T cells function as intermediate precursor exhausted T cells, and fluctuations in the proportions of exhausted T cells and effector T cell populations are associated with the responses to PD-1-based therapies.</p><p>By deciphering the association between the dynamics of ISG-15<sup>+</sup>CD8<sup>+</sup> T cells and clinical response following treatment, the authors discovered that ISG-15<sup>+</sup>CD8<sup>+</sup> T cells could be a significant predictor of a positive treatment response. Their data also revealed that an elevated baseline presence of intratumoral ISG-15<sup>+</sup>CD8<sup>+</sup> T cells may be indicative of a potential benefit from immunochemotherapy. Moreover, ISG15<sup>+</sup>CD8<sup>+</sup> T cell population played a crucial role in the transition to T cell exhaustion, accompanied by escalating levels of LAG-3. In comparison to EBV-negative GC, LAG-3 expression may be upregulated due to an exhaustion expression program triggered by EBV-associated activation. This suggests that LAG-3 could potentially act as a crucial checkpoint for revitalizing the terminal exhausted/dysfunctional T cell subset in EBV-positive GC.</p><p>Moreover, the author described the results of two clinical trials assessing the efficacy of MGD013 and KL-A289 in treating metastatic GC patients. One patient who participated in a phase Ib clinical trial of MGD013, a bi-specific antibody targeting PD-1 and LAG-3, achieved partial response within a month of treatment. Another patient with spleen and multiple lymph node metastases was enrolled in a phase I clinical trial of KL-A289, a LAG-3 inhibitor. After two cycles of KL-A289 treatment, the patient achieved stable disease followed by a significant decrease in the EBV-DNA copy number. These data support further exploration of a LAG-3 antibody in patients with EBV-positive GC and other EBV-associated tumors. Importantly, their longitudinal single-cell view on EBV-positive GC during treatment provided physicians with a direct view on response to treatment, although more detailed investigations on the early effects of anti-LAG-3 and anti-PD-1/PD-L1 are still required. However, the use of biopsies does not allow for direct comparison of the effects of different perturbations, which complicates efforts to answer mechanistic questions. Therefore, alternative approaches that enable direct comparison of the effects of different perturbations should be considered to address this limitation.</p><p>Of note, <i>ex vivo</i> tumor culture systems that maintain the tumor microenvironment and architecture as found in the patient, but that enable perturbation by immunotherapies, offer a unique opportunity to study the dynamics of treatment response and intrinsic properties of a tumor [<span>8</span>]. In particular, air-liquid interface organoids consisting of both tumor and stroma components have been shown to enhance the function of intratumoral T cells on PD-1 blockade [<span>9</span>]. Similarly, various <i>ex vivo</i> models such as patient-derived tumor fragment platform [<span>10</span>], microfluidic cancer-on-chip platform [<span>11</span>], and three-dimensional tumor slice culture platform [<span>12</span>] have been documented with the potential to assess the effect of various antitumor treatment strategies. Using <i>ex vivo</i> tumor culture systems, it is feasible and valuable to assess the effect of anti-LAG3 treatment on the tumor microenvironment and thereby directly test the functional importance of specific cell types in the treatment response.</p><p>Overall, this study represents a significant advancement in our understanding of the EBV-specific tumor immune contexture. The authors propose that the ISG15<sup>+</sup>CD8<sup>+</sup> T cell signature may predict a good response to immunotherapy. More importantly, their findings reveal the necessity of dual blockade of PD-1 and LAG-3 in EBV-associated GC (Figure 1). The comprehensive insights gained from this research pave the way for future research aimed at developing innovative and personalized therapeutic approaches in the fight against cancer.</p><p>Chu-Xia Deng wrote and proofread the manuscript.</p><p>The authors declare that they have no competing interests.</p><p>Not applicable.</p><p>Not applicable.</p>","PeriodicalId":9495,"journal":{"name":"Cancer Communications","volume":"44 4","pages":"491-494"},"PeriodicalIF":24.9000,"publicationDate":"2024-03-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cac2.12529","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Communications","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cac2.12529","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Immune checkpoint inhibitor (ICI) therapy has significantly revolutionized cancer treatment across various malignancies, offering distinct and enduring clinical advantages [1]. Gastric cancer (GC) represents a widespread and life-threatening malignancy with substantial global health implications [2]. However, ICI therapy has not produced satisfactory therapeutic responses in GC patients. Presently, monotherapy targeting the programmed cell death protein 1/programmed death-ligand 1 (PD-1/PD-L1) pathway demonstrates clinical efficacy in approximately 10% of GC patients [3]. Exploration of novel immunotherapeutic targets is urgently needed. Notably, Epstein-Barr virus (EBV)-positive GC constitutes a distinct GC subset, exhibiting a remarkably higher objective response rate to anti-PD-1 inhibitors—an intriguing phenomenon [4]. Several studies have found that EBV-positive GC has more innate and adaptive immune cell infiltration than EBV-negative GC [5, 6]. In their recent publication titled “Dynamic single-cell mapping reveals Epstein-Barr virus-imprinted T-cell exhaustion and on-treatment response”, Qiu et al. [7] unveiled, for the first time, the cellular basis underlying these remarkably heightened responses in EBV-positive GC patients undergoing immunochemotherapy. Leveraging single-cell profiling technologies, this study deepened our comprehension of the intricate and heterogeneous tumor microenvironment in GC.
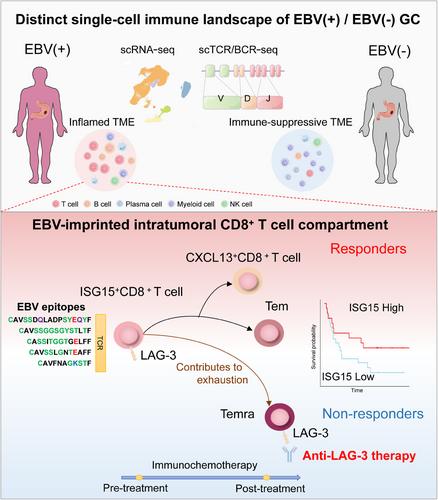
In this study, the authors conducted a comprehensive characterization of the cellular dynamics of tumor-infiltrating immune cells in GC patients, distinguishing between those with EBV-positive and EBV-negative statuses. EBV-positive GC exhibited a heightened immune phenotype characterized by elevated infiltration of T cells and B cells, highlighting the intricate interplay among EBV infection, multi-cellular ecosystems, and tumor development. EBV-negative GC exhibited an immune-suppressive tumor microenvironment characterized by an abundance of plasma cells, myeloid cells, and mast cells. After treatment, the evaluation of the dynamic changes in EBV-positive GC showed an increased presence of cytotoxic CD8+ T cells and effector memory/memory CD8+ T cells. Notably, there was clear evidence of clonal revival and reinvigoration of CD8+ T cells in EBV-positive GC patients, indicating an active T cell-mediated immune reaction enhancing treatment responses.
Furthermore, the authors observed a distinct EBV-imprinted CD8+ T cell population, ISG-15+CD8+ T cells, which exhibited significantly higher expression of interferon-stimulated genes, such as ISG-15, IFIT1-3, RASD2, and MX1. Significantly, ISG-15+CD8+ T cells demonstrated the ability to recognize EBV antigens and coordinated exhausted T cell responses. STARTRAC-tran analysis revealed a robust association between ISG-15+CD8+ T cells and actively proliferating T cells, effector CD8+ T cells (CXCL13+CD8+ T cells) and cytotoxic CD8+ T cells within EBV-positive GC. It is worth mentioning that EBV epitopes were detected within ISG-15+CD8+ T cells, suggesting that this particular cell population consists of T cells specifically targeting EBV. In the context of ICI-responsive GCs, their investigation revealed a significant proportion of ISG-15+CD8+ T clonotypes prior to treatment within the effector T cell populations of EBV-positive tumors after the treatment. In contrast, there was no evidence of re-emerged clonotypes of pre-existing ISG-15+CD8+ T cells in EBV-negative tumors following therapy. More research is required to validate these observations, as these data suggest that ISG-15+CD8+ T cells function as intermediate precursor exhausted T cells, and fluctuations in the proportions of exhausted T cells and effector T cell populations are associated with the responses to PD-1-based therapies.
By deciphering the association between the dynamics of ISG-15+CD8+ T cells and clinical response following treatment, the authors discovered that ISG-15+CD8+ T cells could be a significant predictor of a positive treatment response. Their data also revealed that an elevated baseline presence of intratumoral ISG-15+CD8+ T cells may be indicative of a potential benefit from immunochemotherapy. Moreover, ISG15+CD8+ T cell population played a crucial role in the transition to T cell exhaustion, accompanied by escalating levels of LAG-3. In comparison to EBV-negative GC, LAG-3 expression may be upregulated due to an exhaustion expression program triggered by EBV-associated activation. This suggests that LAG-3 could potentially act as a crucial checkpoint for revitalizing the terminal exhausted/dysfunctional T cell subset in EBV-positive GC.
Moreover, the author described the results of two clinical trials assessing the efficacy of MGD013 and KL-A289 in treating metastatic GC patients. One patient who participated in a phase Ib clinical trial of MGD013, a bi-specific antibody targeting PD-1 and LAG-3, achieved partial response within a month of treatment. Another patient with spleen and multiple lymph node metastases was enrolled in a phase I clinical trial of KL-A289, a LAG-3 inhibitor. After two cycles of KL-A289 treatment, the patient achieved stable disease followed by a significant decrease in the EBV-DNA copy number. These data support further exploration of a LAG-3 antibody in patients with EBV-positive GC and other EBV-associated tumors. Importantly, their longitudinal single-cell view on EBV-positive GC during treatment provided physicians with a direct view on response to treatment, although more detailed investigations on the early effects of anti-LAG-3 and anti-PD-1/PD-L1 are still required. However, the use of biopsies does not allow for direct comparison of the effects of different perturbations, which complicates efforts to answer mechanistic questions. Therefore, alternative approaches that enable direct comparison of the effects of different perturbations should be considered to address this limitation.
Of note, ex vivo tumor culture systems that maintain the tumor microenvironment and architecture as found in the patient, but that enable perturbation by immunotherapies, offer a unique opportunity to study the dynamics of treatment response and intrinsic properties of a tumor [8]. In particular, air-liquid interface organoids consisting of both tumor and stroma components have been shown to enhance the function of intratumoral T cells on PD-1 blockade [9]. Similarly, various ex vivo models such as patient-derived tumor fragment platform [10], microfluidic cancer-on-chip platform [11], and three-dimensional tumor slice culture platform [12] have been documented with the potential to assess the effect of various antitumor treatment strategies. Using ex vivo tumor culture systems, it is feasible and valuable to assess the effect of anti-LAG3 treatment on the tumor microenvironment and thereby directly test the functional importance of specific cell types in the treatment response.
Overall, this study represents a significant advancement in our understanding of the EBV-specific tumor immune contexture. The authors propose that the ISG15+CD8+ T cell signature may predict a good response to immunotherapy. More importantly, their findings reveal the necessity of dual blockade of PD-1 and LAG-3 in EBV-associated GC (Figure 1). The comprehensive insights gained from this research pave the way for future research aimed at developing innovative and personalized therapeutic approaches in the fight against cancer.
Chu-Xia Deng wrote and proofread the manuscript.
The authors declare that they have no competing interests.
期刊介绍:
Cancer Communications is an open access, peer-reviewed online journal that encompasses basic, clinical, and translational cancer research. The journal welcomes submissions concerning clinical trials, epidemiology, molecular and cellular biology, and genetics.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
