Saleh Kaysi, Bakhtar Pacha, Maria Mesquita, Frédéric Collart, Joëlle Nortier
{"title":"Pulmonary congestion and systemic congestion in hemodialysis: dynamics and correlations.","authors":"Saleh Kaysi, Bakhtar Pacha, Maria Mesquita, Frédéric Collart, Joëlle Nortier","doi":"10.3389/fneph.2024.1336863","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Systemic congestion and pulmonary congestion (PC) are common in hemodialysis (HD) patients. However, the relationship between these two entities is not quite clear. We study this relationship and attempt to uncover the factors that may affect it considering different inter-dialytic intervals.</p><p><strong>Methods: </strong>A prospective pilot observational and interventional study including 18 HD patients was conducted. The following were obtained: i) B-line score (BLS) by lung ultrasound (LUS) (reflecting significant pulmonary congestion if BLS > 5), ii) echocardiography, iii) bioelectrical impedance analysis (BIA) (reflecting global volume status), and iv) inferior vena cava (IVC) dynamics (reflecting systemic congestion) before and after the first two consecutive HD sessions of the week, with different inter-dialytic intervals (68 hours and 44 hours). Serum N-terminal pro-brain natriuretic peptide type B (NT-proBNP) levels were obtained before each session. Then, patients were randomized into two groups: the active group, where dry weight was reduced according to BLS + standard of care, and the control group, where dry weight was modified according to standard of care. All the measures were repeated on day 30.</p><p><strong>Results: </strong>We found no correlation between pulmonary congestion represented by BLS and IVC dimensions and dynamics reflecting systemic congestion, independent of different inter-dialytic intervals. Pulmonary congestion was quite prevalent, as mean pre- and post-dialysis BLSs were quite elevated (16 ± 5.53 and 15.3 ± 6.63, respectively) in the first session compared with the second session (16.3 ± 5.26 and 13.6 ± 5.83, respectively). Systolic (left ventricular ejection fraction) and diastolic cardiac function (e/è ratio) parameters from one side and pulmonary congestion (BLS) from the other were not always correlated. BLS was correlated to e/è ratio before HD (session 1) (<i>R</i> <sup>2</sup> = 0.476, <i>p</i> = 0.002) and after HD (session 2) (<i>R</i> <sup>2</sup> = 0.193, <i>p</i> = 0.034). Pulmonary congestion reflected by BLS was correlated to the global volume state reflected by BIA only in the second HD session (HD2) (<i>R</i> <sup>2</sup> = 0.374, <i>p</i> = 0.007). NT-proBNP levels and BLS were correlated before both sessions (<i>R</i> <sup>2</sup> = 0.421, <i>p</i> = 0.004, and <i>R</i> <sup>2</sup> = 0.505, <i>p</i> = 0.001, respectively). Systemic congestion was quite prevalent, as mean pre- and post-dialysis IVC dimensions and dynamics were quite elevated in both sessions, with a higher level of systemic congestion in the first HD session (diameter and collapsibility of 2.1 cm and 23%, and 2.01 cm and 19%, respectively) compared with the second session (1.98 cm and 17.5%, and 1.9 cm and 22%, respectively) without reaching statistical significance. IVC dimensions and global volume status measured by BIA were correlated in the second dialysis session (<i>R</i> <sup>2</sup> = 0.260, <i>p</i> = 0.031). No correlation was found between IVC dimensions and diastolic cardiac function (e/è ratio) parameters or with NT-proBNP levels. On day 30, BLS was significantly reduced in the active group, whereas no difference was found in the control group. However, no real impact was observed on IVC dimensions and dynamics or in total volume status by BIA.</p><p><strong>Conclusion: </strong>Pulmonary congestion is common in HD patients even after reaching their dry weight at the end of two consecutive sessions, and it is not correlated to systemic congestion, suggesting a complex multifactorial pathophysiology origin. Global volume status reflected by BIA and cardiac function are not always related to either systemic congestion represented by IVC dimensions or pulmonary congestion represented by BLS. Fluid redistribution anomalies may allow pulmonary congestion accumulation independently from systemic congestion and global volume status (non-cardiogenic pulmonary congestion). We recommend a personalised approach when managing HD patients by integrating systemic and pulmonary congestion parameters. Dry weight modification guided by repeat LUS may safely reduce pulmonary congestion. However, no impact was observed on systemic congestion or global volume status.</p>","PeriodicalId":73091,"journal":{"name":"Frontiers in nephrology","volume":"4 ","pages":"1336863"},"PeriodicalIF":0.0000,"publicationDate":"2024-02-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10921353/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in nephrology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/fneph.2024.1336863","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Systemic congestion and pulmonary congestion (PC) are common in hemodialysis (HD) patients. However, the relationship between these two entities is not quite clear. We study this relationship and attempt to uncover the factors that may affect it considering different inter-dialytic intervals.
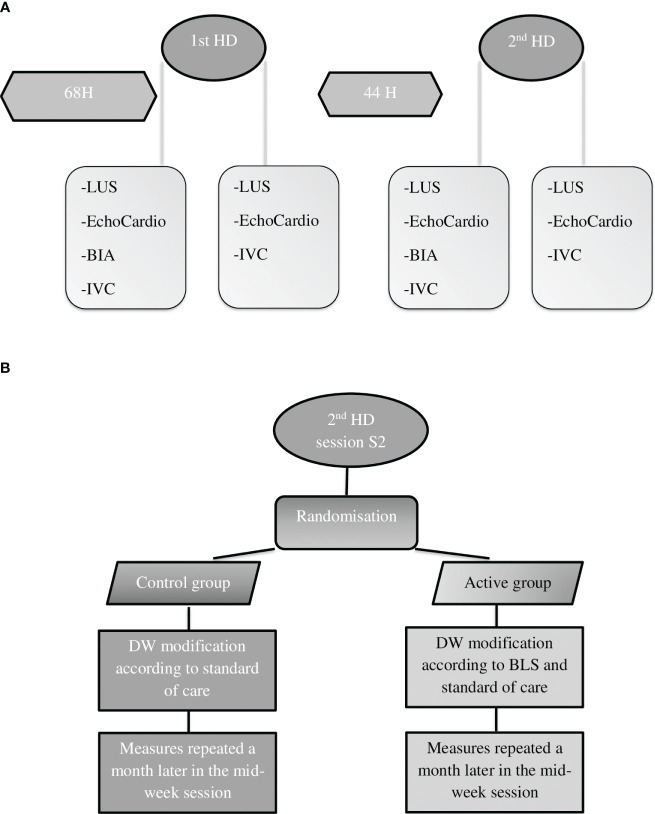
Methods: A prospective pilot observational and interventional study including 18 HD patients was conducted. The following were obtained: i) B-line score (BLS) by lung ultrasound (LUS) (reflecting significant pulmonary congestion if BLS > 5), ii) echocardiography, iii) bioelectrical impedance analysis (BIA) (reflecting global volume status), and iv) inferior vena cava (IVC) dynamics (reflecting systemic congestion) before and after the first two consecutive HD sessions of the week, with different inter-dialytic intervals (68 hours and 44 hours). Serum N-terminal pro-brain natriuretic peptide type B (NT-proBNP) levels were obtained before each session. Then, patients were randomized into two groups: the active group, where dry weight was reduced according to BLS + standard of care, and the control group, where dry weight was modified according to standard of care. All the measures were repeated on day 30.
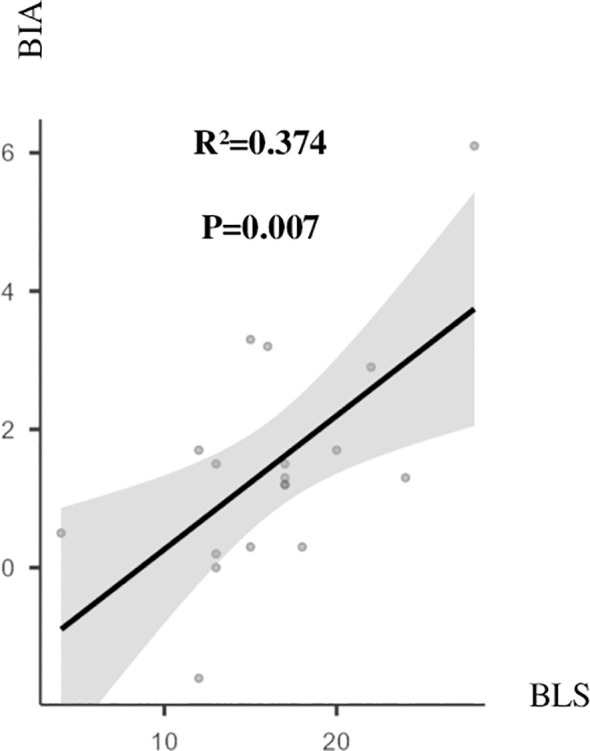
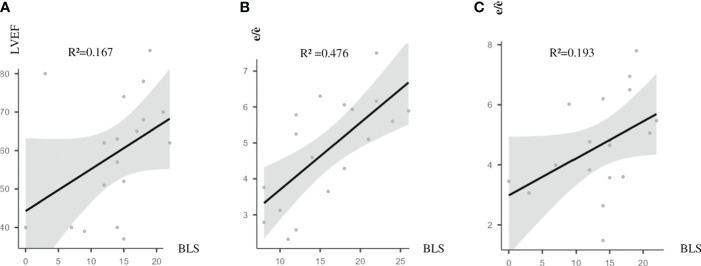
Results: We found no correlation between pulmonary congestion represented by BLS and IVC dimensions and dynamics reflecting systemic congestion, independent of different inter-dialytic intervals. Pulmonary congestion was quite prevalent, as mean pre- and post-dialysis BLSs were quite elevated (16 ± 5.53 and 15.3 ± 6.63, respectively) in the first session compared with the second session (16.3 ± 5.26 and 13.6 ± 5.83, respectively). Systolic (left ventricular ejection fraction) and diastolic cardiac function (e/è ratio) parameters from one side and pulmonary congestion (BLS) from the other were not always correlated. BLS was correlated to e/è ratio before HD (session 1) (R2 = 0.476, p = 0.002) and after HD (session 2) (R2 = 0.193, p = 0.034). Pulmonary congestion reflected by BLS was correlated to the global volume state reflected by BIA only in the second HD session (HD2) (R2 = 0.374, p = 0.007). NT-proBNP levels and BLS were correlated before both sessions (R2 = 0.421, p = 0.004, and R2 = 0.505, p = 0.001, respectively). Systemic congestion was quite prevalent, as mean pre- and post-dialysis IVC dimensions and dynamics were quite elevated in both sessions, with a higher level of systemic congestion in the first HD session (diameter and collapsibility of 2.1 cm and 23%, and 2.01 cm and 19%, respectively) compared with the second session (1.98 cm and 17.5%, and 1.9 cm and 22%, respectively) without reaching statistical significance. IVC dimensions and global volume status measured by BIA were correlated in the second dialysis session (R2 = 0.260, p = 0.031). No correlation was found between IVC dimensions and diastolic cardiac function (e/è ratio) parameters or with NT-proBNP levels. On day 30, BLS was significantly reduced in the active group, whereas no difference was found in the control group. However, no real impact was observed on IVC dimensions and dynamics or in total volume status by BIA.
Conclusion: Pulmonary congestion is common in HD patients even after reaching their dry weight at the end of two consecutive sessions, and it is not correlated to systemic congestion, suggesting a complex multifactorial pathophysiology origin. Global volume status reflected by BIA and cardiac function are not always related to either systemic congestion represented by IVC dimensions or pulmonary congestion represented by BLS. Fluid redistribution anomalies may allow pulmonary congestion accumulation independently from systemic congestion and global volume status (non-cardiogenic pulmonary congestion). We recommend a personalised approach when managing HD patients by integrating systemic and pulmonary congestion parameters. Dry weight modification guided by repeat LUS may safely reduce pulmonary congestion. However, no impact was observed on systemic congestion or global volume status.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
