Pedro Abreu, Manuel Correia, Elsa Azevedo, Bernardo Sousa-Pinto, Rui Magalhães
{"title":"Rapid systematic review of readmissions costs after stroke.","authors":"Pedro Abreu, Manuel Correia, Elsa Azevedo, Bernardo Sousa-Pinto, Rui Magalhães","doi":"10.1186/s12962-024-00518-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Stroke readmissions are considered a marker of health quality and may pose a burden to healthcare systems. However, information on the costs of post-stroke readmissions has not been systematically reviewed.</p><p><strong>Objectives: </strong>To systematically review information about the costs of hospital readmissions of patients whose primary diagnosis in the index admission was a stroke.</p><p><strong>Methods: </strong>A rapid systematic review was performed on studies reporting post-stroke readmission costs in EMBASE, MEDLINE, and Web of Science up to June 2021. Relevant data were extracted and presented by readmission and stroke type. The original study's currency values were converted to 2021 US dollars based on the purchasing power parity for gross domestic product. The reporting quality of each of the included studies was assessed using the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) checklist.</p><p><strong>Results: </strong>Forty-four studies were identified. Considerable variability in readmission costs was observed among countries, readmissions, stroke types, and durations of the follow-up period. The UK and the USA were the countries reporting the highest readmission costs. In the first year of follow-up, stroke readmission costs accounted for 2.1-23.4%, of direct costs and 3.3-21% of total costs. Among the included studies, only one identified predictors of readmission costs.</p><p><strong>Conclusion: </strong>Our review showed great variability in readmission costs, mainly due to differences in study design, countries and health services, follow-up duration, and reported readmission data. The results of this study can be used to inform policymakers and healthcare providers about the burden of stroke readmissions. Future studies should not solely focus on improving data standardization but should also prioritize the identification of stroke readmission cost predictors.</p>","PeriodicalId":47054,"journal":{"name":"Cost Effectiveness and Resource Allocation","volume":"22 1","pages":"22"},"PeriodicalIF":2.5000,"publicationDate":"2024-03-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10936094/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cost Effectiveness and Resource Allocation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12962-024-00518-3","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH POLICY & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Stroke readmissions are considered a marker of health quality and may pose a burden to healthcare systems. However, information on the costs of post-stroke readmissions has not been systematically reviewed.
Objectives: To systematically review information about the costs of hospital readmissions of patients whose primary diagnosis in the index admission was a stroke.
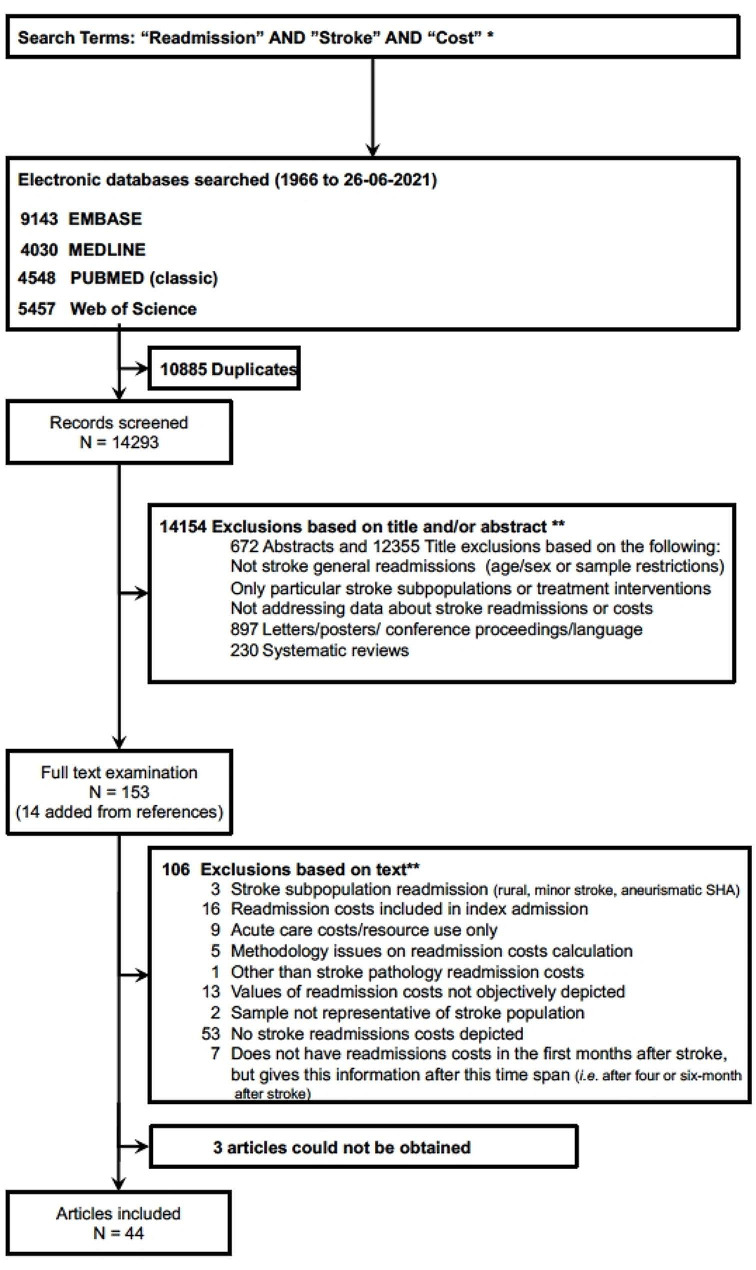
Methods: A rapid systematic review was performed on studies reporting post-stroke readmission costs in EMBASE, MEDLINE, and Web of Science up to June 2021. Relevant data were extracted and presented by readmission and stroke type. The original study's currency values were converted to 2021 US dollars based on the purchasing power parity for gross domestic product. The reporting quality of each of the included studies was assessed using the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) checklist.
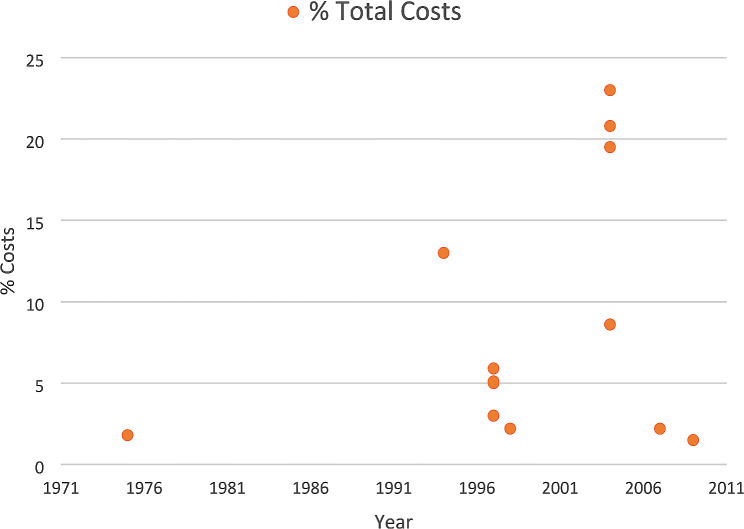
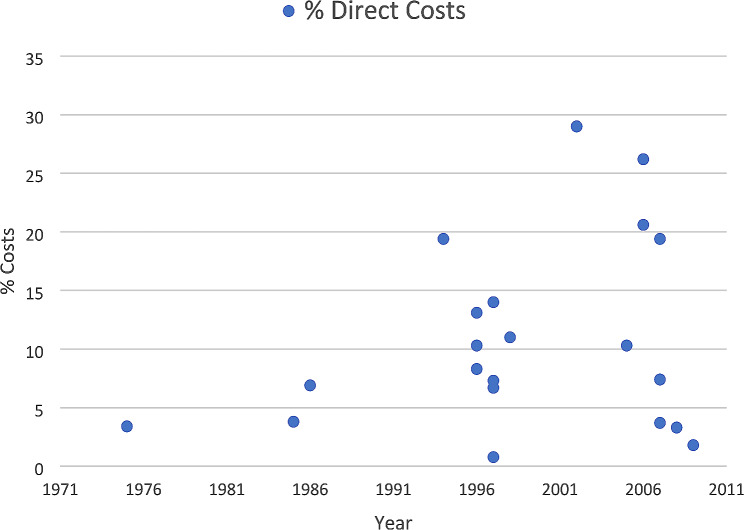
Results: Forty-four studies were identified. Considerable variability in readmission costs was observed among countries, readmissions, stroke types, and durations of the follow-up period. The UK and the USA were the countries reporting the highest readmission costs. In the first year of follow-up, stroke readmission costs accounted for 2.1-23.4%, of direct costs and 3.3-21% of total costs. Among the included studies, only one identified predictors of readmission costs.
Conclusion: Our review showed great variability in readmission costs, mainly due to differences in study design, countries and health services, follow-up duration, and reported readmission data. The results of this study can be used to inform policymakers and healthcare providers about the burden of stroke readmissions. Future studies should not solely focus on improving data standardization but should also prioritize the identification of stroke readmission cost predictors.
期刊介绍:
Cost Effectiveness and Resource Allocation is an Open Access, peer-reviewed, online journal that considers manuscripts on all aspects of cost-effectiveness analysis, including conceptual or methodological work, economic evaluations, and policy analysis related to resource allocation at a national or international level. Cost Effectiveness and Resource Allocation is aimed at health economists, health services researchers, and policy-makers with an interest in enhancing the flow and transfer of knowledge relating to efficiency in the health sector. Manuscripts are encouraged from researchers based in low- and middle-income countries, with a view to increasing the international economic evidence base for health.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
