Outcome and Risk of Poststroke Pneumonia in Patients with Acute Ischemic Stroke After Endovascular Thrombectomy: A Post Hoc Analysis of the DIRECT-MT Trial.
Ping Zhang, Lei Chen, Xiao-Fei Ye, Tao Wu, Ben-Qiang Deng, Peng-Fei Yang, Yi Han, Yong-Wei Zhang, Jian-Min Liu
{"title":"Outcome and Risk of Poststroke Pneumonia in Patients with Acute Ischemic Stroke After Endovascular Thrombectomy: A Post Hoc Analysis of the DIRECT-MT Trial.","authors":"Ping Zhang, Lei Chen, Xiao-Fei Ye, Tao Wu, Ben-Qiang Deng, Peng-Fei Yang, Yi Han, Yong-Wei Zhang, Jian-Min Liu","doi":"10.1007/s12028-024-01947-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In this study, we aimed to investigate the risk factors and impact of poststroke pneumonia (PSP) on mortality and functional outcome in patients with acute ischemic stroke (AIS) after endovascular thrombectomy (EVT).</p><p><strong>Methods: </strong>This was a post hoc analysis of a prospective randomized trial (Direct intraarterial thrombectomy in order to revascularize AIS patients with large-vessel occlusion efficiently in Chinese tertiary hospitals: a multicenter randomized clinical trial). Patients with AIS who completed EVT were evaluated for the occurrence of PSP during the hospitalization period and their modified Rankin Scale (mRS) scores at 90 days after AIS. Logistic regression analysis was conducted to investigate the independent predictors of PSP. Propensity score matching was conducted for the PSP and non-PSP groups by using the covariates resulting from the logistic regression analysis. The associations between PSP and outcomes were analyzed. The outcomes included 90-day poor functional outcome (mRS scores > 2), 90-day mortality, and early 2-week mortality.</p><p><strong>Results: </strong>A total of 639 patients were enrolled, of whom 29.58% (189) developed PSP. Logistic regression analysis revealed that history of chronic heart failure (unadjusted odds ratio [OR] 2.011, 95% confidence interval [CI] 1.026-3.941; P = 0.042), prethrombectomy reperfusion on initial digital subtraction angiography (OR 0.394, 95% CI 0.161-0.964; P = 0.041), creatinine levels at admission (OR 1.008, 95% CI 1.000-1.016; P = 0.049), and National Institutes of Health Stroke Scale at 24 h (OR 1.023, 95% CI 1.007-1.039; P = 0.004) were independent risk factors for PSP. With propensity scoring matching, poor functional outcome (mRS > 2) was more common in patients with PSP than in patients without PSP (81.03% vs. 71.83%, P = 0.043) at 90 days after EVT. The early 2-week mortality of patients with PSP was lower (5.74% vs. 12.07%, P = 0.038). But there was no statistically significant difference in 90-day mortality between the PSP group and non-PSP group (22.41% vs. 14.94%, P = 0.074). The survivorship curve also shows no statistical significance (P = 0.088) between the two groups.</p><p><strong>Conclusions: </strong>Nearly one third of patients with AIS and EVT developed PSP. Heart failure, higher creatinine levels, prethrombectomy reperfusion, and National Institutes of Health Stroke Scale at 24 h were associated with PSP in these patients. PSP was associated with poor 90-day functional outcomes in patients with AIS treated with EVT.</p>","PeriodicalId":19118,"journal":{"name":"Neurocritical Care","volume":" ","pages":"489-497"},"PeriodicalIF":3.6000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurocritical Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s12028-024-01947-x","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/13 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: In this study, we aimed to investigate the risk factors and impact of poststroke pneumonia (PSP) on mortality and functional outcome in patients with acute ischemic stroke (AIS) after endovascular thrombectomy (EVT).
Methods: This was a post hoc analysis of a prospective randomized trial (Direct intraarterial thrombectomy in order to revascularize AIS patients with large-vessel occlusion efficiently in Chinese tertiary hospitals: a multicenter randomized clinical trial). Patients with AIS who completed EVT were evaluated for the occurrence of PSP during the hospitalization period and their modified Rankin Scale (mRS) scores at 90 days after AIS. Logistic regression analysis was conducted to investigate the independent predictors of PSP. Propensity score matching was conducted for the PSP and non-PSP groups by using the covariates resulting from the logistic regression analysis. The associations between PSP and outcomes were analyzed. The outcomes included 90-day poor functional outcome (mRS scores > 2), 90-day mortality, and early 2-week mortality.
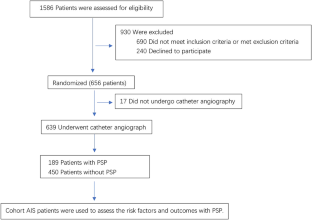
Results: A total of 639 patients were enrolled, of whom 29.58% (189) developed PSP. Logistic regression analysis revealed that history of chronic heart failure (unadjusted odds ratio [OR] 2.011, 95% confidence interval [CI] 1.026-3.941; P = 0.042), prethrombectomy reperfusion on initial digital subtraction angiography (OR 0.394, 95% CI 0.161-0.964; P = 0.041), creatinine levels at admission (OR 1.008, 95% CI 1.000-1.016; P = 0.049), and National Institutes of Health Stroke Scale at 24 h (OR 1.023, 95% CI 1.007-1.039; P = 0.004) were independent risk factors for PSP. With propensity scoring matching, poor functional outcome (mRS > 2) was more common in patients with PSP than in patients without PSP (81.03% vs. 71.83%, P = 0.043) at 90 days after EVT. The early 2-week mortality of patients with PSP was lower (5.74% vs. 12.07%, P = 0.038). But there was no statistically significant difference in 90-day mortality between the PSP group and non-PSP group (22.41% vs. 14.94%, P = 0.074). The survivorship curve also shows no statistical significance (P = 0.088) between the two groups.
Conclusions: Nearly one third of patients with AIS and EVT developed PSP. Heart failure, higher creatinine levels, prethrombectomy reperfusion, and National Institutes of Health Stroke Scale at 24 h were associated with PSP in these patients. PSP was associated with poor 90-day functional outcomes in patients with AIS treated with EVT.
期刊介绍:
Neurocritical Care is a peer reviewed scientific publication whose major goal is to disseminate new knowledge on all aspects of acute neurological care. It is directed towards neurosurgeons, neuro-intensivists, neurologists, anesthesiologists, emergency physicians, and critical care nurses treating patients with urgent neurologic disorders. These are conditions that may potentially evolve rapidly and could need immediate medical or surgical intervention. Neurocritical Care provides a comprehensive overview of current developments in intensive care neurology, neurosurgery and neuroanesthesia and includes information about new therapeutic avenues and technological innovations. Neurocritical Care is the official journal of the Neurocritical Care Society.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
