A Scoping Review of Personalized, Interactive, Web-Based Clinical Decision Tools Available for Breast Cancer Prevention and Screening in the United States.
Dalya Kamil, Kaitlyn M Wojcik, Laney Smith, Julia Zhang, Oliver W A Wilson, Gisela Butera, Jinani Jayasekera
{"title":"A Scoping Review of Personalized, Interactive, Web-Based Clinical Decision Tools Available for Breast Cancer Prevention and Screening in the United States.","authors":"Dalya Kamil, Kaitlyn M Wojcik, Laney Smith, Julia Zhang, Oliver W A Wilson, Gisela Butera, Jinani Jayasekera","doi":"10.1177/23814683241236511","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction.</b> Personalized web-based clinical decision tools for breast cancer prevention and screening could address knowledge gaps, enhance patient autonomy in shared decision-making, and promote equitable care. The purpose of this review was to present evidence on the availability, usability, feasibility, acceptability, quality, and uptake of breast cancer prevention and screening tools to support their integration into clinical care. <b>Methods.</b> We used the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews Checklist to conduct this review. We searched 6 databases to identify literature on the development, validation, usability, feasibility, acceptability testing, and uptake of the tools into practice settings. Quality assessment for each tool was conducted using the International Patient Decision Aid Standard instrument, with quality scores ranging from 0 to 63 (lowest-highest). <b>Results.</b> We identified 10 tools for breast cancer prevention and 9 tools for screening. The tools included individual (e.g., age), clinical (e.g., genomic risk factors), and health behavior (e.g., alcohol use) characteristics. Fourteen tools included race/ethnicity, but no tool incorporated contextual factors (e.g., insurance, access) associated with breast cancer. All tools were internally or externally validated. Six tools had undergone usability testing in samples including White (median, 71%; range, 9%-96%), insured (99%; 97%-100%) women, with college education or higher (60%; 27%-100%). All of the tools were developed and tested in academic settings. Seven (37%) tools showed potential evidence of uptake in clinical practice. The tools had an average quality assessment score of 21 (range, 9-39). <b>Conclusions.</b> There is limited evidence on testing and uptake of breast cancer prevention and screening tools in diverse clinical settings. The development, testing, and integration of tools in academic and nonacademic settings could potentially improve uptake and equitable access to these tools.</p><p><strong>Highlights: </strong>There were 19 personalized, interactive, Web-based decision tools for breast cancer prevention and screening.Breast cancer outcomes were personalized based on individual clinical characteristics (e.g., age, medical history), genomic risk factors (e.g., BRCA1/2), race and ethnicity, and health behaviors (e.g., smoking). The tools did not include contextual factors (e.g., insurance status, access to screening facilities) that could potentially contribute to breast cancer outcomes.Validation, usability, acceptability, and feasibility testing were conducted mostly among White and/or insured patients with some college education (or higher) in academic settings. There was limited evidence on testing and uptake of the tools in nonacademic clinical settings.</p>","PeriodicalId":36567,"journal":{"name":"MDM Policy and Practice","volume":"9 1","pages":"23814683241236511"},"PeriodicalIF":1.7000,"publicationDate":"2024-03-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10946080/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"MDM Policy and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/23814683241236511","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
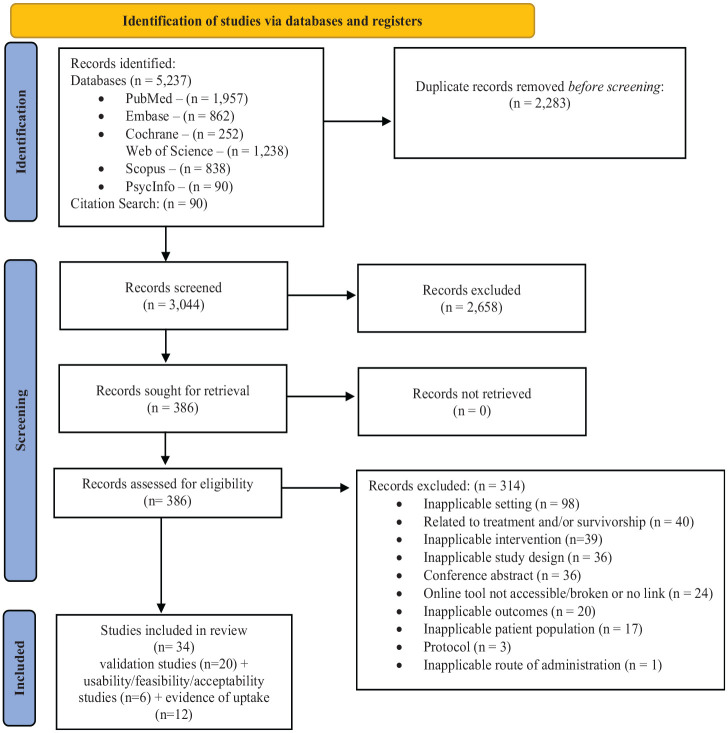
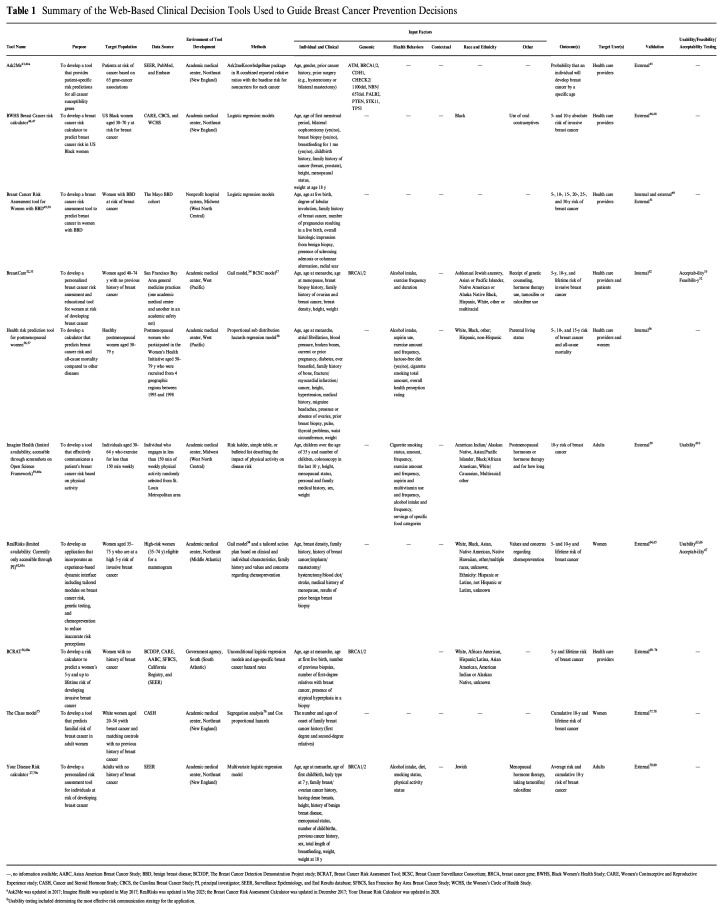
Introduction. Personalized web-based clinical decision tools for breast cancer prevention and screening could address knowledge gaps, enhance patient autonomy in shared decision-making, and promote equitable care. The purpose of this review was to present evidence on the availability, usability, feasibility, acceptability, quality, and uptake of breast cancer prevention and screening tools to support their integration into clinical care. Methods. We used the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews Checklist to conduct this review. We searched 6 databases to identify literature on the development, validation, usability, feasibility, acceptability testing, and uptake of the tools into practice settings. Quality assessment for each tool was conducted using the International Patient Decision Aid Standard instrument, with quality scores ranging from 0 to 63 (lowest-highest). Results. We identified 10 tools for breast cancer prevention and 9 tools for screening. The tools included individual (e.g., age), clinical (e.g., genomic risk factors), and health behavior (e.g., alcohol use) characteristics. Fourteen tools included race/ethnicity, but no tool incorporated contextual factors (e.g., insurance, access) associated with breast cancer. All tools were internally or externally validated. Six tools had undergone usability testing in samples including White (median, 71%; range, 9%-96%), insured (99%; 97%-100%) women, with college education or higher (60%; 27%-100%). All of the tools were developed and tested in academic settings. Seven (37%) tools showed potential evidence of uptake in clinical practice. The tools had an average quality assessment score of 21 (range, 9-39). Conclusions. There is limited evidence on testing and uptake of breast cancer prevention and screening tools in diverse clinical settings. The development, testing, and integration of tools in academic and nonacademic settings could potentially improve uptake and equitable access to these tools.
Highlights: There were 19 personalized, interactive, Web-based decision tools for breast cancer prevention and screening.Breast cancer outcomes were personalized based on individual clinical characteristics (e.g., age, medical history), genomic risk factors (e.g., BRCA1/2), race and ethnicity, and health behaviors (e.g., smoking). The tools did not include contextual factors (e.g., insurance status, access to screening facilities) that could potentially contribute to breast cancer outcomes.Validation, usability, acceptability, and feasibility testing were conducted mostly among White and/or insured patients with some college education (or higher) in academic settings. There was limited evidence on testing and uptake of the tools in nonacademic clinical settings.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
