{"title":"Differentiating gallbladder cancer from polyps using non-enhanced magnetic resonance imaging.","authors":"Kazuyoshi Ohki, Takao Igarashi, Hiroyuki Yakabe, Megumi Shiraishi, Takayuki Suzuki, Jun Woo, Hiroya Ojiri","doi":"10.5114/pjr.2024.135730","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>This retrospective cohort study assessed the efficiency of non-enhanced magnetic resonance imaging (MRI) for differentiating gallbladder cancer (GBC) from gallbladder polyps (GBPs) measuring ≥ 10 mm.</p><p><strong>Material and methods: </strong>Patients diagnosed with GBCs or GBPs ≥ 10 mm and GBC ≤ T2 stage were eligible for inclusion. Two independent blinded readers assessed the continuity of the mucosal and muscular layers (CMML; present or absent) and normalised signal intensity ratio (NIR) on the apparent diffusion coefficient map (NIR-ADC), T1-weighted image (NIR-T1WI), and T2-weighted half-Fourier acquisition single-shot turbo spin-echo image. Univariate and multivariate logistic regression analyses and interobserver agreement analyses were performed to detect predictive variables differentiating GBCs from GBPs. Receiver operating characteristic (ROC) analysis was performed to evaluate diagnostic performance. A reproducibility test was performed to verify the predictive variables.</p><p><strong>Results: </strong>Multivariate analysis showed significant differences in CMML, NIR-ADC, and NIR-T1WI (<i>p</i> < 0.001). The positive predictive value (PPV) and specificity of the absence of CMML were approximately 100%. The CMML showed the best specificity, accuracy, and PPV in the reproducibility study. The sensitivity of CMML alone was approximately 50%, whereas it increased to approximately 70% when combined with NIR-ADC. The diagnostic performance of the combination, including sensitivity, was almost like that of tumour size. The combined tumour size and CMML assessment showed higher diagnostic performance than tumour size alone.</p><p><strong>Conclusions: </strong>The absence of CMML and NIR-ADC ≤ 1.86 helped in differentiating GBCs from GBPs. Evaluation of the absence of CMML and measurement of tumour size could better aid in determining between the two than measurement of tumour size alone.</p>","PeriodicalId":94174,"journal":{"name":"Polish journal of radiology","volume":"89 ","pages":"e106-e114"},"PeriodicalIF":0.0000,"publicationDate":"2024-02-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10953508/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Polish journal of radiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5114/pjr.2024.135730","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: This retrospective cohort study assessed the efficiency of non-enhanced magnetic resonance imaging (MRI) for differentiating gallbladder cancer (GBC) from gallbladder polyps (GBPs) measuring ≥ 10 mm.
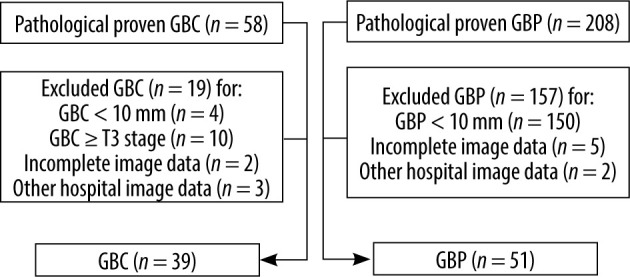
Material and methods: Patients diagnosed with GBCs or GBPs ≥ 10 mm and GBC ≤ T2 stage were eligible for inclusion. Two independent blinded readers assessed the continuity of the mucosal and muscular layers (CMML; present or absent) and normalised signal intensity ratio (NIR) on the apparent diffusion coefficient map (NIR-ADC), T1-weighted image (NIR-T1WI), and T2-weighted half-Fourier acquisition single-shot turbo spin-echo image. Univariate and multivariate logistic regression analyses and interobserver agreement analyses were performed to detect predictive variables differentiating GBCs from GBPs. Receiver operating characteristic (ROC) analysis was performed to evaluate diagnostic performance. A reproducibility test was performed to verify the predictive variables.
Results: Multivariate analysis showed significant differences in CMML, NIR-ADC, and NIR-T1WI (p < 0.001). The positive predictive value (PPV) and specificity of the absence of CMML were approximately 100%. The CMML showed the best specificity, accuracy, and PPV in the reproducibility study. The sensitivity of CMML alone was approximately 50%, whereas it increased to approximately 70% when combined with NIR-ADC. The diagnostic performance of the combination, including sensitivity, was almost like that of tumour size. The combined tumour size and CMML assessment showed higher diagnostic performance than tumour size alone.
Conclusions: The absence of CMML and NIR-ADC ≤ 1.86 helped in differentiating GBCs from GBPs. Evaluation of the absence of CMML and measurement of tumour size could better aid in determining between the two than measurement of tumour size alone.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
