In-hospital mortality after prehospital endotracheal intubation versus alternative methods of airway management in trauma patients. A cohort study from the TraumaRegister DGU®.
Moritz Weigeldt, Stefan Schulz-Drost, Dirk Stengel, Rolf Lefering, Sascha Treskatsch, Christian Berger
{"title":"In-hospital mortality after prehospital endotracheal intubation versus alternative methods of airway management in trauma patients. A cohort study from the TraumaRegister DGU®.","authors":"Moritz Weigeldt, Stefan Schulz-Drost, Dirk Stengel, Rolf Lefering, Sascha Treskatsch, Christian Berger","doi":"10.1007/s00068-024-02498-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Prehospital airway management in trauma is a key component of care and is associated with particular risks. Endotracheal intubation (ETI) is the gold standard, while extraglottic airway devices (EGAs) are recommended alternatives. There is limited evidence comparing their effectiveness. In this retrospective analysis from the TraumaRegister DGU®, we compared ETI with EGA in prehospital airway management regarding in-hospital mortality in patients with trauma.</p><p><strong>Methods: </strong>We included cases only from German hospitals with a minimum Abbreviated Injury Scale score ≥ 2 and age ≥ 16 years. All patients without prehospital airway protection were excluded. We performed a multivariate logistic regression to adjust with the outcome measure of hospital mortality.</p><p><strong>Results: </strong>We included n = 10,408 cases of whom 92.5% received ETI and 7.5% EGA. The mean injury severity score was higher in the ETI group (28.8 ± 14.2) than in the EGA group (26.3 ± 14.2), and in-hospital mortality was comparable: ETI 33.0%; EGA 30.7% (27.5 to 33.9). After conducting logistic regression, the odds ratio for mortality in the ETI group was 1.091 (0.87 to 1.37). The standardized mortality ratio was 1.04 (1.01 to 1.07) in the ETI group and 1.1 (1.02 to 1.26) in the EGA group.</p><p><strong>Conclusions: </strong>There was no significant difference in mortality rates between the use of ETI or EGA, or the ratio of expected versus observed mortality when using ETI.</p>","PeriodicalId":12064,"journal":{"name":"European Journal of Trauma and Emergency Surgery","volume":" ","pages":"1637-1647"},"PeriodicalIF":2.2000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11458629/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Trauma and Emergency Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00068-024-02498-8","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/20 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Prehospital airway management in trauma is a key component of care and is associated with particular risks. Endotracheal intubation (ETI) is the gold standard, while extraglottic airway devices (EGAs) are recommended alternatives. There is limited evidence comparing their effectiveness. In this retrospective analysis from the TraumaRegister DGU®, we compared ETI with EGA in prehospital airway management regarding in-hospital mortality in patients with trauma.
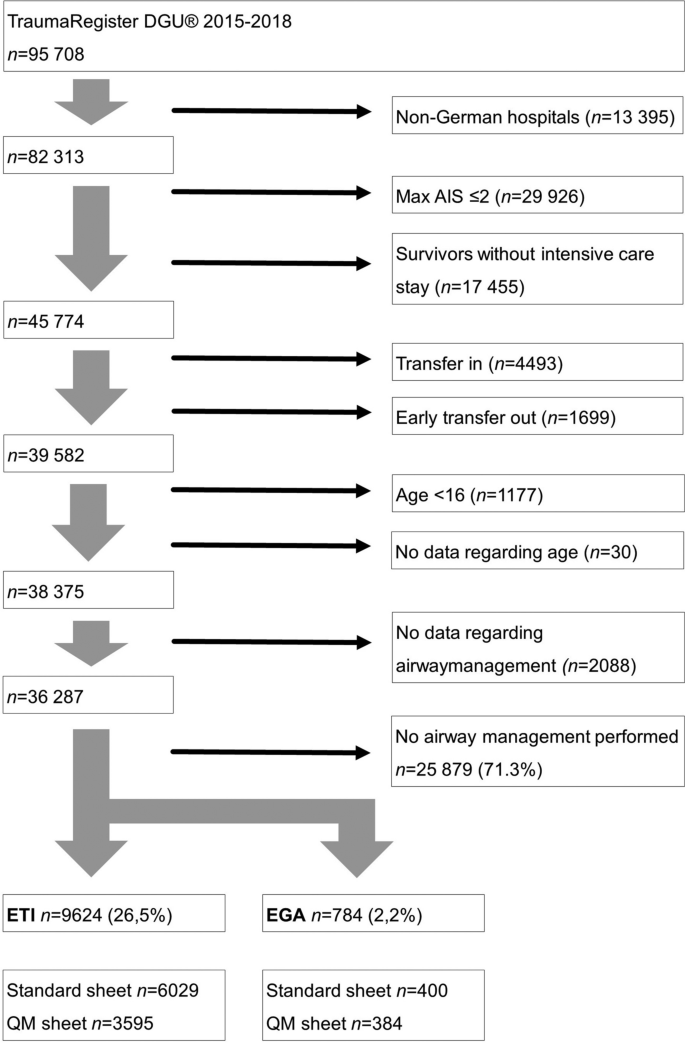
Methods: We included cases only from German hospitals with a minimum Abbreviated Injury Scale score ≥ 2 and age ≥ 16 years. All patients without prehospital airway protection were excluded. We performed a multivariate logistic regression to adjust with the outcome measure of hospital mortality.
Results: We included n = 10,408 cases of whom 92.5% received ETI and 7.5% EGA. The mean injury severity score was higher in the ETI group (28.8 ± 14.2) than in the EGA group (26.3 ± 14.2), and in-hospital mortality was comparable: ETI 33.0%; EGA 30.7% (27.5 to 33.9). After conducting logistic regression, the odds ratio for mortality in the ETI group was 1.091 (0.87 to 1.37). The standardized mortality ratio was 1.04 (1.01 to 1.07) in the ETI group and 1.1 (1.02 to 1.26) in the EGA group.
Conclusions: There was no significant difference in mortality rates between the use of ETI or EGA, or the ratio of expected versus observed mortality when using ETI.
期刊介绍:
The European Journal of Trauma and Emergency Surgery aims to open an interdisciplinary forum that allows for the scientific exchange between basic and clinical science related to pathophysiology, diagnostics and treatment of traumatized patients. The journal covers all aspects of clinical management, operative treatment and related research of traumatic injuries.
Clinical and experimental papers on issues relevant for the improvement of trauma care are published. Reviews, original articles, short communications and letters allow the appropriate presentation of major and minor topics.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
