Marine Van Hollebeke, Karan Chohan, Colin J Adams, Jolene H Fisher, Shane Shapera, Lee Fidler, Ewan C Goligher, Tereza Martinu, Lisa Wickerson, Sunita Mathur, Lianne G Singer, W Darlene Reid, Dmitry Rozenberg
{"title":"Clinical implications of frailty assessed in hospitalized patients with acute-exacerbation of interstitial lung disease.","authors":"Marine Van Hollebeke, Karan Chohan, Colin J Adams, Jolene H Fisher, Shane Shapera, Lee Fidler, Ewan C Goligher, Tereza Martinu, Lisa Wickerson, Sunita Mathur, Lianne G Singer, W Darlene Reid, Dmitry Rozenberg","doi":"10.1177/14799731241240786","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Approximately 50% of patients with interstitial lung disease (ILD) experience frailty, which remains unexplored in acute exacerbations of ILD (AE-ILD). A better understanding may help with prognostication and resource planning. We evaluated the association of frailty with clinical characteristics, physical function, hospital outcomes, and post-AE-ILD recovery.</p><p><strong>Methods: </strong>Retrospective cohort study of AE-ILD patients (01/2015-10/2019) with frailty (proportion ≥0.25) on a 30-item cumulative-deficits index. Frail and non-frail patients were compared for pre- and post-hospitalization clinical characteristics, adjusted for age, sex, and ILD diagnosis. One-year mortality, considering transplantation as a competing risk, was analysed adjusting for age, frailty, and Charlson Comorbidity Index (CCI).</p><p><strong>Results: </strong>89 AE-ILD patients were admitted (median: 67 years, 63% idiopathic pulmonary fibrosis). 31 were frail, which was associated with older age, greater CCI, lower 6-min walk distance, and decreased independence pre-hospitalization. Frail patients had more major complications (32% vs 10%, <i>p</i> = .01) and required more multidisciplinary support during hospitalization. Frailty was not associated with 1-year mortality (HR: 0.97, 95%CI: [0.45-2.10]) factoring transplantation as a competing risk.</p><p><strong>Conclusions: </strong>Frailty was associated with reduced exercise capacity, increased comorbidities and hospital complications. Identifying frailty may highlight those requiring additional multidisciplinary support, but further study is needed to explore whether frailty is modifiable with AE-ILD.</p>","PeriodicalId":10217,"journal":{"name":"Chronic Respiratory Disease","volume":"21 ","pages":"14799731241240786"},"PeriodicalIF":2.3000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10958799/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chronic Respiratory Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/14799731241240786","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Approximately 50% of patients with interstitial lung disease (ILD) experience frailty, which remains unexplored in acute exacerbations of ILD (AE-ILD). A better understanding may help with prognostication and resource planning. We evaluated the association of frailty with clinical characteristics, physical function, hospital outcomes, and post-AE-ILD recovery.
Methods: Retrospective cohort study of AE-ILD patients (01/2015-10/2019) with frailty (proportion ≥0.25) on a 30-item cumulative-deficits index. Frail and non-frail patients were compared for pre- and post-hospitalization clinical characteristics, adjusted for age, sex, and ILD diagnosis. One-year mortality, considering transplantation as a competing risk, was analysed adjusting for age, frailty, and Charlson Comorbidity Index (CCI).
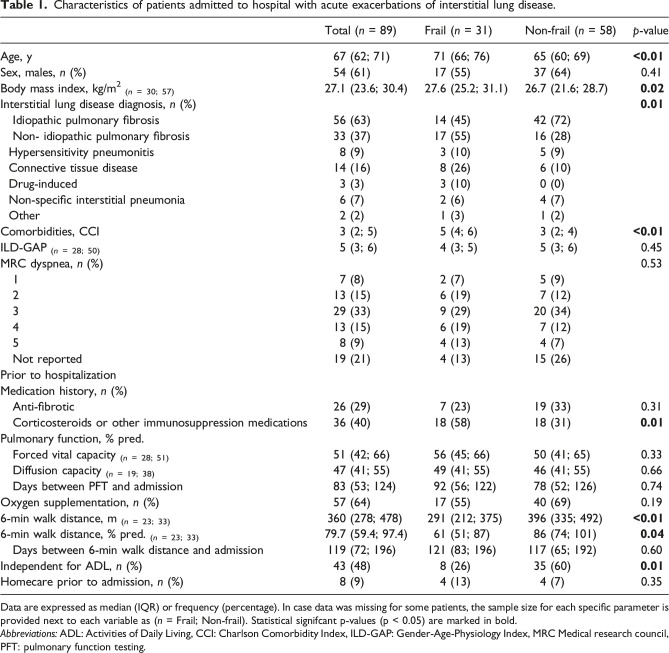
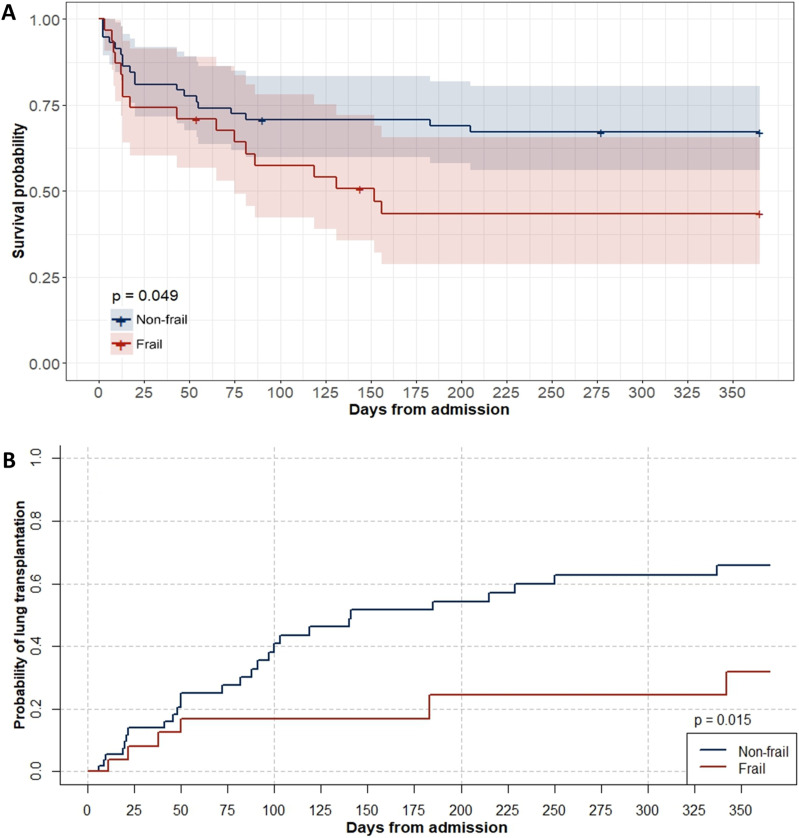
Results: 89 AE-ILD patients were admitted (median: 67 years, 63% idiopathic pulmonary fibrosis). 31 were frail, which was associated with older age, greater CCI, lower 6-min walk distance, and decreased independence pre-hospitalization. Frail patients had more major complications (32% vs 10%, p = .01) and required more multidisciplinary support during hospitalization. Frailty was not associated with 1-year mortality (HR: 0.97, 95%CI: [0.45-2.10]) factoring transplantation as a competing risk.
Conclusions: Frailty was associated with reduced exercise capacity, increased comorbidities and hospital complications. Identifying frailty may highlight those requiring additional multidisciplinary support, but further study is needed to explore whether frailty is modifiable with AE-ILD.
期刊介绍:
Chronic Respiratory Disease is a peer-reviewed, open access, scholarly journal, created in response to the rising incidence of chronic respiratory diseases worldwide. It publishes high quality research papers and original articles that have immediate relevance to clinical practice and its multi-disciplinary perspective reflects the nature of modern treatment. The journal provides a high quality, multi-disciplinary focus for the publication of original papers, reviews and commentary in the broad area of chronic respiratory disease, particularly its treatment and management.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
