Douglas R. Nordli III, Stephanie Burkhalter, Kaila Fives, Fernando Galan
{"title":"A dramatic EEG response to fenfluramine in a patient with developmental and epileptic encephalopathy","authors":"Douglas R. Nordli III, Stephanie Burkhalter, Kaila Fives, Fernando Galan","doi":"10.1002/cns3.20060","DOIUrl":null,"url":null,"abstract":"<p>We describe a remarkable electroencephalographic (EEG) response in a boy with intractable epilepsy and developmental and epileptic encephalopathy (DEE). Although there are studies on seizure control with fenfluramine in patients with Dravet syndrome (DS) and Lennox-Gastaut syndrome (LGS), no publications on other DEEs exist. The dramatic EEG improvement following fenfluramine initiation has not been described in individuals with DS or LGS. Our report highlights these novel findings with the hope of encouraging more research into fenfluramine's use in patients with difficult-to-treat epilepsies and DEEs.</p><p>This 3-year-old, right-handed boy with intractable focal epilepsy and DEE was admitted to the epilepsy monitoring unit (EMU) for EEG characterization. His seizures began at age 2 years and initially occurred more than eight times per day. The predominant seizure type was described as generalized tonic to tonic-clonic, which initally occurred on average once per week. Other seizure types included hyperkinetic generalized tonic-clonic seizures, focal motor hemifacial clonic seizures, and frequent generalized myoclonic seizures.</p><p>His EEG studies revealed a disorganized and slow background with superimposed multifocal pleomorphic epileptiform discharges. While admitted to the EMU for seizure characterization, fenfluramine was initiated. The baseline EEG (Figure 1A,B) was similar to his prior EEG recordings and revealed samples of his awake and asleep EEG background. His magnetic resonance imaging scan was normal. Genetic testing, including an epilepsy gene panel and whole-exome sequencing, were nondiagnostic.</p><p>Previous medications included levetiracetam, ethosuximide, and valproic acid. Current medications consisted of Federal Drug Administration–approved cannabidiol, lacosamide, and clobazam at therapeutic doses.</p><p>The boy's history was remarkable for developmental delay, and his examination was otherwise nonfocal. During the EMU admission he was started on fenfluramine (0.2 mg/kg/day) as an adjunct to his current regimen. A baseline EEG recording was obtained on the first day of admission after which fenfluramine (0.2 mg/kg/day divided twice daily) was started, with a robust response noted on EEG within 24–48 hours of starting fenfluramine (Figure 2A,B).</p><p>We present a pediatric patient with refractory epilepsy and DEE who demonstrated a dramatic EEG response after the initiation of fenfluramine (0.2 mg/kg/day). Fenfluramine has shown efficacy in seizure control in patients with DS and LGS, but dramatic responses trending toward EEG normalization have not been described in these patients.<span><sup>1, 2</sup></span> Interestingly, researchers studying the use of fenfluramine in sunflower syndrome also documented an EEG response as well as clinical improvement in several patients. One patient exhibited improved slowing, while focal background slowing improved in two patients. Additionally, epileptiform discharges resolved in two patients, and two individuals who initially experienced seizures on EEG were seizure-free after initiating fenfluramine.<span><sup>3</sup></span></p><p>Our patient is now seizure-free, and his development is improving seven months after initiation of fenfluramine. The etiology of his epilepsy, however, remains unknown, despite extensive efforts to identify it. Advanced diagnostic measures including whole-genome sequencing are being considered.</p><p>This novel report indicates the need for further investigation into both fenfluramine's ability to treat epileptic encephalopathy and other types of epilepsies with deleterious patterns outside of DS and LGS. Our patient is still under active investigation and follow-up. We describe him to draw attention to this remarkable finding in the hopes of sharing this signal with other physicians and patients who may benefit from the use of fenfluramine outside of patients with DS and LGS. This report is limited in that it describes a single patient with an unclear etiology of epilepsy. We hope that if other dramatic responses are documented, we can better understand the mechanism responsible for this remarkable finding.</p><p><b>Douglas R. Nordli</b>: Conceptualization; writing—original draft; writing—review and editing. <b>Stephanie Burkhalter</b>: Data curation. <b>Kaila Fives</b>: Writing—original draft; writing—review and editing. <b>Fernando Galan</b>: Conceptualization; writing—review and editing.</p><p>The authors declare no conflicts of interest.</p>","PeriodicalId":72232,"journal":{"name":"Annals of the Child Neurology Society","volume":"2 1","pages":"82-85"},"PeriodicalIF":0.0000,"publicationDate":"2024-03-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cns3.20060","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of the Child Neurology Society","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cns3.20060","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
We describe a remarkable electroencephalographic (EEG) response in a boy with intractable epilepsy and developmental and epileptic encephalopathy (DEE). Although there are studies on seizure control with fenfluramine in patients with Dravet syndrome (DS) and Lennox-Gastaut syndrome (LGS), no publications on other DEEs exist. The dramatic EEG improvement following fenfluramine initiation has not been described in individuals with DS or LGS. Our report highlights these novel findings with the hope of encouraging more research into fenfluramine's use in patients with difficult-to-treat epilepsies and DEEs.
This 3-year-old, right-handed boy with intractable focal epilepsy and DEE was admitted to the epilepsy monitoring unit (EMU) for EEG characterization. His seizures began at age 2 years and initially occurred more than eight times per day. The predominant seizure type was described as generalized tonic to tonic-clonic, which initally occurred on average once per week. Other seizure types included hyperkinetic generalized tonic-clonic seizures, focal motor hemifacial clonic seizures, and frequent generalized myoclonic seizures.
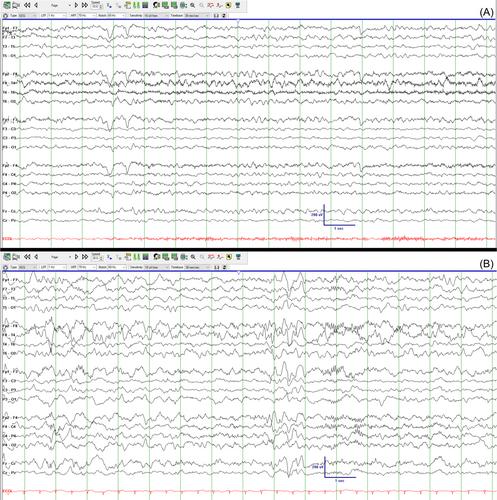
His EEG studies revealed a disorganized and slow background with superimposed multifocal pleomorphic epileptiform discharges. While admitted to the EMU for seizure characterization, fenfluramine was initiated. The baseline EEG (Figure 1A,B) was similar to his prior EEG recordings and revealed samples of his awake and asleep EEG background. His magnetic resonance imaging scan was normal. Genetic testing, including an epilepsy gene panel and whole-exome sequencing, were nondiagnostic.
Previous medications included levetiracetam, ethosuximide, and valproic acid. Current medications consisted of Federal Drug Administration–approved cannabidiol, lacosamide, and clobazam at therapeutic doses.
The boy's history was remarkable for developmental delay, and his examination was otherwise nonfocal. During the EMU admission he was started on fenfluramine (0.2 mg/kg/day) as an adjunct to his current regimen. A baseline EEG recording was obtained on the first day of admission after which fenfluramine (0.2 mg/kg/day divided twice daily) was started, with a robust response noted on EEG within 24–48 hours of starting fenfluramine (Figure 2A,B).
We present a pediatric patient with refractory epilepsy and DEE who demonstrated a dramatic EEG response after the initiation of fenfluramine (0.2 mg/kg/day). Fenfluramine has shown efficacy in seizure control in patients with DS and LGS, but dramatic responses trending toward EEG normalization have not been described in these patients.1, 2 Interestingly, researchers studying the use of fenfluramine in sunflower syndrome also documented an EEG response as well as clinical improvement in several patients. One patient exhibited improved slowing, while focal background slowing improved in two patients. Additionally, epileptiform discharges resolved in two patients, and two individuals who initially experienced seizures on EEG were seizure-free after initiating fenfluramine.3
Our patient is now seizure-free, and his development is improving seven months after initiation of fenfluramine. The etiology of his epilepsy, however, remains unknown, despite extensive efforts to identify it. Advanced diagnostic measures including whole-genome sequencing are being considered.
This novel report indicates the need for further investigation into both fenfluramine's ability to treat epileptic encephalopathy and other types of epilepsies with deleterious patterns outside of DS and LGS. Our patient is still under active investigation and follow-up. We describe him to draw attention to this remarkable finding in the hopes of sharing this signal with other physicians and patients who may benefit from the use of fenfluramine outside of patients with DS and LGS. This report is limited in that it describes a single patient with an unclear etiology of epilepsy. We hope that if other dramatic responses are documented, we can better understand the mechanism responsible for this remarkable finding.
Douglas R. Nordli: Conceptualization; writing—original draft; writing—review and editing. Stephanie Burkhalter: Data curation. Kaila Fives: Writing—original draft; writing—review and editing. Fernando Galan: Conceptualization; writing—review and editing.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
