Eficacia del bloqueo retrolaminar ecoguiado frente al bloqueo paravertebral clásico en pacientes sometidos a hernioplastia inguinal unilateral: estudio controlado aleatorizado
{"title":"Eficacia del bloqueo retrolaminar ecoguiado frente al bloqueo paravertebral clásico en pacientes sometidos a hernioplastia inguinal unilateral: estudio controlado aleatorizado","authors":"","doi":"10.1016/j.redar.2024.01.005","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><div>In daily surgical practice, inguinal hernioplasty is a frequent procedure that is frequently accompanied by severe postoperative pain. Multiple regional blocks have been described for analgesia after such operations. Retrolaminar block (RLB) is a paravertebral block (PVB) variant that provides excellent analgesia and reduces the risk of complications. This prospective trial compared the analgesic efficacy of PVB and RLB in the inguinal hernioplasty.</div></div><div><h3>Methods</h3><div>The 56 patients included were randomly assigned into two equal groups according to the block performed under ultrasound guidance at the T12 level: PVB group (28 patients) and RLB (28 patients). Time until the first rescue analgesia was our primary outcome. Other outcomes included the time to perform the block, changes in intraoperative hemodynamic parameters, postoperative VAS, 24-hour morphine consumption, the level of patient satisfaction, and the incidence of block-related complications.</div></div><div><h3>Results</h3><div>Demographic data were comparable in the two groups. However, the time needed for the block was significantly shortened with the RLB (p<!--> <!--><<!--> <!-->0.001). Patients in the PVB groups expressed better pain scores and lower opioid consumption. Additionally, the time to the first call for opioid analgesia showed a significant prolongation in association with the PVB. There was no discernible difference in the frequency of adverse events and recorded MAP and HR.</div></div><div><h3>Conclusion</h3><div>The PVB has a superior perioperative analgesic profile compared to the RLB, which manifested in the prolonged duration to the first rescue analgesics, better pain scores, and less opioid consumption, with no significant increase in block-related complications.</div></div>","PeriodicalId":46479,"journal":{"name":"Revista Espanola de Anestesiologia y Reanimacion","volume":"71 8","pages":"Pages 584-591"},"PeriodicalIF":0.8000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Revista Espanola de Anestesiologia y Reanimacion","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0034935624000483","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background
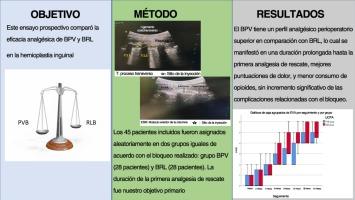
In daily surgical practice, inguinal hernioplasty is a frequent procedure that is frequently accompanied by severe postoperative pain. Multiple regional blocks have been described for analgesia after such operations. Retrolaminar block (RLB) is a paravertebral block (PVB) variant that provides excellent analgesia and reduces the risk of complications. This prospective trial compared the analgesic efficacy of PVB and RLB in the inguinal hernioplasty.
Methods
The 56 patients included were randomly assigned into two equal groups according to the block performed under ultrasound guidance at the T12 level: PVB group (28 patients) and RLB (28 patients). Time until the first rescue analgesia was our primary outcome. Other outcomes included the time to perform the block, changes in intraoperative hemodynamic parameters, postoperative VAS, 24-hour morphine consumption, the level of patient satisfaction, and the incidence of block-related complications.
Results
Demographic data were comparable in the two groups. However, the time needed for the block was significantly shortened with the RLB (p < 0.001). Patients in the PVB groups expressed better pain scores and lower opioid consumption. Additionally, the time to the first call for opioid analgesia showed a significant prolongation in association with the PVB. There was no discernible difference in the frequency of adverse events and recorded MAP and HR.
Conclusion
The PVB has a superior perioperative analgesic profile compared to the RLB, which manifested in the prolonged duration to the first rescue analgesics, better pain scores, and less opioid consumption, with no significant increase in block-related complications.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
