This study aimed to investigate the radiological, pathological, and prognostic characteristics of large consolidative-type pulmonary invasive mucinous adenocarcinomas (IMA).
We retrospectively reviewed 738 patients who confirmed IMA between January 2010 and August 2022, and two radiologists reviewed imaging data to determine subtypes. We included 41 patients with pathologically large consolidative-type IMA. We analyzed their radiological, pathological, and prognostic characteristics. The recurrence-free survival (RFS) and overall survival (OS) were determined using the Kaplan–Meier method.
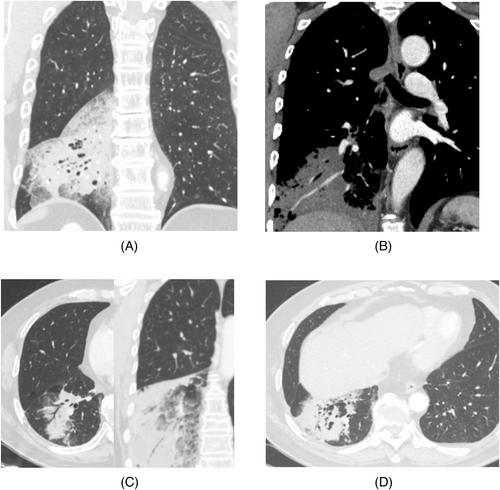
Most lesions were located in the lower lobe, with 46.3% patients showing multiple lesions. Halo, angiogram, vacuole, air bronchogram, and dead branch sign were observed in 97.6%, 73.2%, 63.4%, 61.0%, and 61.0% of the cases, respectively. Unevenly low enhancement was observed in 88.89% of patients. T3 and T4 pathological stages were observed in 50.0% and 30.6% of patients, respectively. Lymph node metastasis was observed in 16.7% patients, with no distant metastasis. Spread-through air spaces and intrapulmonary dissemination were observed in 27.8% and 19.4% patients, respectively. Moreover, Kirsten rat sarcoma viral oncogene mutations were found in 68.6% of cases, and no epidermal growth factor receptor mutations were seen. Among all mutation sites, G12V mutation is the most common, accounting for 40%. The average RFS and OS were 19.4 and 66.4 months, respectively, with 3-year RFS and OS rates of 30.0% and 75.0%, respectively. Pleural invasion and lymph node metastasis were independent risk factors for diagnosis.
Halo, vacuole, angiogram, and dead branch signs were frequently observed in consolidative-type IMA. Kirsten rat sarcoma viral oncogene mutations are common in consolidative-type IMA, especially site G12V, whereas epidermal growth factor receptor mutations were rare; therefore, gene immunotherapy was more difficult. Most patients were in stage T3–T4; however, lymph node metastasis was rare.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
