Immune cell pair ratio captured by imaging mass cytometry has superior predictive value for prognosis of non-small cell lung cancer than cell fraction and density
{"title":"Immune cell pair ratio captured by imaging mass cytometry has superior predictive value for prognosis of non-small cell lung cancer than cell fraction and density","authors":"Jian-Rong Li, Chao Cheng","doi":"10.1002/cac2.12540","DOIUrl":null,"url":null,"abstract":"<p>Infiltrating immune cells in the tumor microenvironment (TME) play critical roles in the initiation, progression, and metastasis of cancer [<span>1</span>]. Previous studies have reported that the infiltration levels of various immune cell types are significantly associated with patient prognosis in different cancers [<span>2, 3</span>]. Specifically, in non-small cell lung cancer (NSCLC) the prognostic associations of major immune cell types have been investigated [<span>4-6</span>], however, some of the reported associations are inconsistent and remain debated [<span>7</span>]. Limited by technical issues, most studies focused on a few immune cell lineages or relied on inferred immune cell levels from computational deconvolution. To investigate the prognostic effects of all major immune cell types unbiasedly, more systematic high-quality immune cell profiling data with matched patient survival information are needed.</p><p>Recently, Sorin <i>et al.</i> [<span>8</span>] used imaging mass cytometry (IMC) to characterize the immunological landscape of 416 distinct lung adenocarcinoma (LUAD) samples at single-cell resolution. The IMC images provide the counts and spatial distribution of 16 cell types with high precision in each sample. These cell types include cancer and endothelial cells, along with 14 immune cell types, including CD163<sup>+</sup> and CD163<sup>−</sup> macrophages, CD8<sup>+</sup>, CD4<sup>+</sup>, regulatory, and other T cells, classical, non-classical, and intermediate monocytes, natural killer cells, dendritic cells, mast cells, neutrophils, and other immune cells. Additionally, the data provide patient survival and other clinical information. Using these data, we investigated the prognostic associations of the cell density (#cells/megapixel) and fractions of the 16 cell types as well as the fraction ratio between each pair of cell types (Supplementary Methods). Our results indicated that the relative abundance between cell types (fraction ratios) was more prognostic than cell fractions and densities.</p><p>We calculated the densities of the 16 cell types in each patient's IMC image and applied Cox regression analysis to examine their associations with progression-free survival (PFS) after adjusting for established clinical factors including age, sex, smoking status, and tumor stage. At the significance level of <i>P</i> < 0.05, only the density of non-classical monocytes was found to have a significant association with worse prognosis (hazard ratio [HR] = 1.004, <i>P</i> = 0.040, Figure 1A). After multiple testing corrections, none of the cell types was significant (false discovery rate [FDR] > 0.05). Similar results were obtained when cell fractions among all cells were used for prognostic association analysis (Figure 1B). In addition, we conducted prognostic analysis on 14 immune cell types, focusing on their proportions among immune cells (excluding cancer and endothelial cells), yielding similar results. It has been well-known that some cell types play more immune suppressive toles in the TME, while others are more stimulatory. We therefore investigated the prognostic effect of relative abundance between different cell types. For each pair of the 16 cell types we calculated the ratio of their cell fractions (equal to the ratio of cell densities). From these ratios, we identified 28 cell pairs significantly associated with PFS (<i>P</i> < 0.05), adjusted for clinical factors (Figure 1C). After multiple testing corrections, 9 pairs remained significant (FDR < 0.05). As an example, the non-classical monocyte/CD4<sup>+</sup> T cell ratio was associated with a significantly worse PFS (<i>P</i> < 0.001). We conducted a multivariable Cox regression model incorporating the fractions of non-classical monocytes, CD4<sup>+</sup> T cells, their ratio, and various clinical factors. The result indicated that neither non-classical monocytes nor CD4<sup>+</sup> T cells was significant, but the non-classical monocyte/CD4<sup>+</sup> T cell ratio was significantly associated with a shorter PFS (Figure 1D). Similar results were obtained when overall survival (OS) was used: cell-cell ratios were more prognostic than cell fractions and densities (Figure 1E and Supplementary Figure S1). Further analysis revealed significant associations of T other/CD4<sup>+</sup> T cell and non-classical monocyte/CD4<sup>+</sup> T cell ratios with advanced stages or male patients and of the CD8<sup>+</sup> T cell/cancer cell ratio with smoking or patients under 75 years old (Supplementary Figure S2), highlighting these clinical factors' prognostic impact.</p><p>By connecting all significant cell-cell pairs, we established a prognostic cell-cell interaction network, providing an overview of key pairs. Figure 1F illustrates a significant association of LUAD progression with the ratios of both infiltrating non-classical monocytes and their precursor intermediate monocytes to both CD8<sup>+</sup> and CD4<sup>+</sup> T cells. Additionally, higher ratios of infiltrating non-classical monocytes, intermediate monocytes, CD163<sup>+</sup> macrophages, and other T cells to B cells, CD8<sup>+</sup> T cells, or CD4<sup>+</sup> T cells, were linked to poorer OS (Supplementary Figure S3). These results highlight the pivotal prognostic role of the ratio of non-classical or intermediate monocytes to CD4<sup>+</sup> or CD8<sup>+</sup> T cells in LUAD, consistent with previous studies showing that non-classical or intermediate monocytes suppressed the proliferation and immune responses of CD8<sup>+</sup> or CD4<sup>+</sup> T cells [<span>9, 10</span>].</p><p>To further consolidate our results, we performed down-sampling analyses 100 times, each time randomly selecting 80% of samples for prognostic analysis. For cell density and cell fraction, the numbers of cell types significantly associated with PFS (FDR < 0.05) were only 0.01 and 0.02 on average, respectively (Supplementary Figure S4A). In contrast, an average of 9.37 significant cell-cell pairs was identified. Additionally, we down-sampled cells from all images by randomly selecting 80% of cells and recalculated cell fractions for prognostic analysis, repeated 100 times. On average, 9.74 significant cell-cell pairs were identified each time, while no significant associations were found using cell fraction and cell density (Supplementary Figure S4B). These findings suggest that the greater prognostic relevance of relative cell abundances over cell density/fraction was not merely due to a limited subset of patient samples or cells.</p><p>In conclusion, our study established that in LUAD, the prognostic value was more closely associated with the relative abundances between specific cell types within the TME than with the absolute cell densities or fractions depicted by IMC images. This finding underscores the prognostic significance of interactions between distinct immune cells in the TME, especially the immunological equilibrium between immunosuppressive and immunostimulatory cells. Such insights have significant implications for the development of targeted therapies and patient stratification in LUAD, based on the nuanced understanding of immune cell interactions.</p><p>Chao Cheng designed the study. Jian-Rong Li collected the dataset. Chao Cheng and Jian-Rong Li performed the analysis. Jian-Rong Li constructed the figures. Chao Cheng and Jian-Rong Li interpret results and wrote the manuscript. Chao Cheng supervised the project. All authors provided feedback, revisions, and input on the final manuscript.</p><p>The authors declare no competing financial interests.</p><p>This study is supported by the Cancer Prevention Research Institute of Texas (CPRIT) (RR180061 to CC) and the National Cancer Institute of the National Institute of Health (1R01CA269764 to CC). CC is a CPRIT Scholar in Cancer Research.</p><p>Not applicable</p>","PeriodicalId":9495,"journal":{"name":"Cancer Communications","volume":"44 5","pages":"589-592"},"PeriodicalIF":24.9000,"publicationDate":"2024-03-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cac2.12540","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Communications","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cac2.12540","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Infiltrating immune cells in the tumor microenvironment (TME) play critical roles in the initiation, progression, and metastasis of cancer [1]. Previous studies have reported that the infiltration levels of various immune cell types are significantly associated with patient prognosis in different cancers [2, 3]. Specifically, in non-small cell lung cancer (NSCLC) the prognostic associations of major immune cell types have been investigated [4-6], however, some of the reported associations are inconsistent and remain debated [7]. Limited by technical issues, most studies focused on a few immune cell lineages or relied on inferred immune cell levels from computational deconvolution. To investigate the prognostic effects of all major immune cell types unbiasedly, more systematic high-quality immune cell profiling data with matched patient survival information are needed.
Recently, Sorin et al. [8] used imaging mass cytometry (IMC) to characterize the immunological landscape of 416 distinct lung adenocarcinoma (LUAD) samples at single-cell resolution. The IMC images provide the counts and spatial distribution of 16 cell types with high precision in each sample. These cell types include cancer and endothelial cells, along with 14 immune cell types, including CD163+ and CD163− macrophages, CD8+, CD4+, regulatory, and other T cells, classical, non-classical, and intermediate monocytes, natural killer cells, dendritic cells, mast cells, neutrophils, and other immune cells. Additionally, the data provide patient survival and other clinical information. Using these data, we investigated the prognostic associations of the cell density (#cells/megapixel) and fractions of the 16 cell types as well as the fraction ratio between each pair of cell types (Supplementary Methods). Our results indicated that the relative abundance between cell types (fraction ratios) was more prognostic than cell fractions and densities.
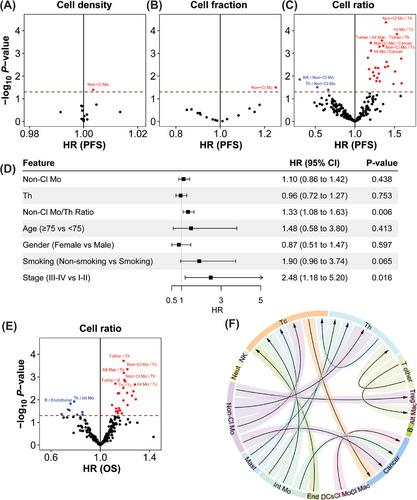
We calculated the densities of the 16 cell types in each patient's IMC image and applied Cox regression analysis to examine their associations with progression-free survival (PFS) after adjusting for established clinical factors including age, sex, smoking status, and tumor stage. At the significance level of P < 0.05, only the density of non-classical monocytes was found to have a significant association with worse prognosis (hazard ratio [HR] = 1.004, P = 0.040, Figure 1A). After multiple testing corrections, none of the cell types was significant (false discovery rate [FDR] > 0.05). Similar results were obtained when cell fractions among all cells were used for prognostic association analysis (Figure 1B). In addition, we conducted prognostic analysis on 14 immune cell types, focusing on their proportions among immune cells (excluding cancer and endothelial cells), yielding similar results. It has been well-known that some cell types play more immune suppressive toles in the TME, while others are more stimulatory. We therefore investigated the prognostic effect of relative abundance between different cell types. For each pair of the 16 cell types we calculated the ratio of their cell fractions (equal to the ratio of cell densities). From these ratios, we identified 28 cell pairs significantly associated with PFS (P < 0.05), adjusted for clinical factors (Figure 1C). After multiple testing corrections, 9 pairs remained significant (FDR < 0.05). As an example, the non-classical monocyte/CD4+ T cell ratio was associated with a significantly worse PFS (P < 0.001). We conducted a multivariable Cox regression model incorporating the fractions of non-classical monocytes, CD4+ T cells, their ratio, and various clinical factors. The result indicated that neither non-classical monocytes nor CD4+ T cells was significant, but the non-classical monocyte/CD4+ T cell ratio was significantly associated with a shorter PFS (Figure 1D). Similar results were obtained when overall survival (OS) was used: cell-cell ratios were more prognostic than cell fractions and densities (Figure 1E and Supplementary Figure S1). Further analysis revealed significant associations of T other/CD4+ T cell and non-classical monocyte/CD4+ T cell ratios with advanced stages or male patients and of the CD8+ T cell/cancer cell ratio with smoking or patients under 75 years old (Supplementary Figure S2), highlighting these clinical factors' prognostic impact.
By connecting all significant cell-cell pairs, we established a prognostic cell-cell interaction network, providing an overview of key pairs. Figure 1F illustrates a significant association of LUAD progression with the ratios of both infiltrating non-classical monocytes and their precursor intermediate monocytes to both CD8+ and CD4+ T cells. Additionally, higher ratios of infiltrating non-classical monocytes, intermediate monocytes, CD163+ macrophages, and other T cells to B cells, CD8+ T cells, or CD4+ T cells, were linked to poorer OS (Supplementary Figure S3). These results highlight the pivotal prognostic role of the ratio of non-classical or intermediate monocytes to CD4+ or CD8+ T cells in LUAD, consistent with previous studies showing that non-classical or intermediate monocytes suppressed the proliferation and immune responses of CD8+ or CD4+ T cells [9, 10].
To further consolidate our results, we performed down-sampling analyses 100 times, each time randomly selecting 80% of samples for prognostic analysis. For cell density and cell fraction, the numbers of cell types significantly associated with PFS (FDR < 0.05) were only 0.01 and 0.02 on average, respectively (Supplementary Figure S4A). In contrast, an average of 9.37 significant cell-cell pairs was identified. Additionally, we down-sampled cells from all images by randomly selecting 80% of cells and recalculated cell fractions for prognostic analysis, repeated 100 times. On average, 9.74 significant cell-cell pairs were identified each time, while no significant associations were found using cell fraction and cell density (Supplementary Figure S4B). These findings suggest that the greater prognostic relevance of relative cell abundances over cell density/fraction was not merely due to a limited subset of patient samples or cells.
In conclusion, our study established that in LUAD, the prognostic value was more closely associated with the relative abundances between specific cell types within the TME than with the absolute cell densities or fractions depicted by IMC images. This finding underscores the prognostic significance of interactions between distinct immune cells in the TME, especially the immunological equilibrium between immunosuppressive and immunostimulatory cells. Such insights have significant implications for the development of targeted therapies and patient stratification in LUAD, based on the nuanced understanding of immune cell interactions.
Chao Cheng designed the study. Jian-Rong Li collected the dataset. Chao Cheng and Jian-Rong Li performed the analysis. Jian-Rong Li constructed the figures. Chao Cheng and Jian-Rong Li interpret results and wrote the manuscript. Chao Cheng supervised the project. All authors provided feedback, revisions, and input on the final manuscript.
The authors declare no competing financial interests.
This study is supported by the Cancer Prevention Research Institute of Texas (CPRIT) (RR180061 to CC) and the National Cancer Institute of the National Institute of Health (1R01CA269764 to CC). CC is a CPRIT Scholar in Cancer Research.
期刊介绍:
Cancer Communications is an open access, peer-reviewed online journal that encompasses basic, clinical, and translational cancer research. The journal welcomes submissions concerning clinical trials, epidemiology, molecular and cellular biology, and genetics.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
