Anne M Sydor, Emily Bergin, Jonathan Kay, Erik Stone, Robert Popovian
{"title":"Modeling the Effects of Formulary Exclusions: How Many Patients Could Be Affected by a Specific Exclusion?","authors":"Anne M Sydor, Emily Bergin, Jonathan Kay, Erik Stone, Robert Popovian","doi":"10.36469/001c.94544","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Medication formularies, initially designed to promote the use of cost-effective generic drugs, are now designed to maximize financial benefits for the pharmacy benefit management companies that negotiate purchase prices. In the second-largest pharmacy benefit management formulary that is publicly available, 55% of mandated substitutions are not for generic or biosimilar versions of the same active ingredient and/or formulation and may not be medically or financially beneficial to patients. <b>Methods:</b> We modeled the effect of excluding novel agents for atrial fibrillation/venous thromboembolism, migraine prevention, and psoriasis, which all would require substitution with a different active ingredient. Using population data, market share of the 2 largest US formularies, and 2021 prescription data, we calculated how many people could be affected by such exclusions. Using data from the published literature, we calculated how many of those individuals are likely to discontinue treatment and/or have adverse events due to a formulary exclusion. <b>Results:</b> The number of people likely to have adverse events due to the exclusion could be as high as 1 million for atrial fibrillation/venous thromboembolism, 900 000 for migraine prevention, and 500 000 for psoriasis. The numbers likely to discontinue treatment for their condition are as high as 924 000 for atrial fibrillation/venous thromboembolism, 646 000 for migraine, and 138 000 for psoriasis. <b>Conclusion:</b> Substitution with a nonequivalent treatment is common in formularies currently in use and is not without substantial consequences for hundreds of thousands of patients. Forced medication substitution results in costly increases in morbidity and mortality and should be part of the cost-benefit analysis of any formulary exclusion.</p>","PeriodicalId":16012,"journal":{"name":"Journal of Health Economics and Outcomes Research","volume":"11 1","pages":"86-93"},"PeriodicalIF":2.3000,"publicationDate":"2024-03-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10970716/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Health Economics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36469/001c.94544","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
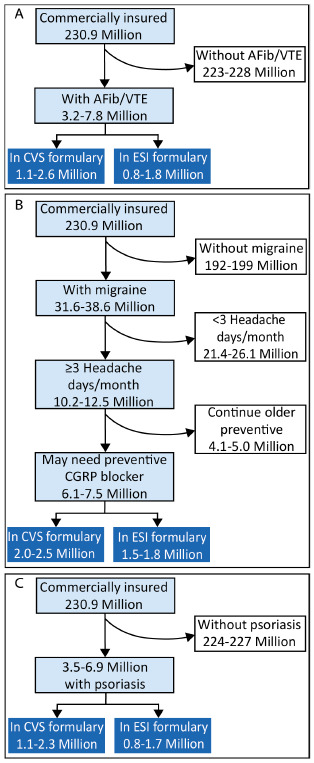
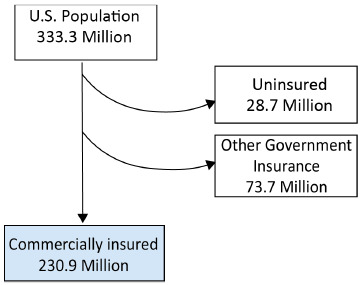
Background: Medication formularies, initially designed to promote the use of cost-effective generic drugs, are now designed to maximize financial benefits for the pharmacy benefit management companies that negotiate purchase prices. In the second-largest pharmacy benefit management formulary that is publicly available, 55% of mandated substitutions are not for generic or biosimilar versions of the same active ingredient and/or formulation and may not be medically or financially beneficial to patients. Methods: We modeled the effect of excluding novel agents for atrial fibrillation/venous thromboembolism, migraine prevention, and psoriasis, which all would require substitution with a different active ingredient. Using population data, market share of the 2 largest US formularies, and 2021 prescription data, we calculated how many people could be affected by such exclusions. Using data from the published literature, we calculated how many of those individuals are likely to discontinue treatment and/or have adverse events due to a formulary exclusion. Results: The number of people likely to have adverse events due to the exclusion could be as high as 1 million for atrial fibrillation/venous thromboembolism, 900 000 for migraine prevention, and 500 000 for psoriasis. The numbers likely to discontinue treatment for their condition are as high as 924 000 for atrial fibrillation/venous thromboembolism, 646 000 for migraine, and 138 000 for psoriasis. Conclusion: Substitution with a nonequivalent treatment is common in formularies currently in use and is not without substantial consequences for hundreds of thousands of patients. Forced medication substitution results in costly increases in morbidity and mortality and should be part of the cost-benefit analysis of any formulary exclusion.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
