Fabian M Troschel, Benjamin O Troschel, Maren Kloss, Johanna Jost, Niklas B Pepper, Amelie S Völk-Troschel, Rainer G Wiewrodt, Walter Stummer, Dorothee Wiewrodt, Hans Theodor Eich
{"title":"Sarcopenia is associated with chemoradiotherapy discontinuation and reduced progression-free survival in glioblastoma patients.","authors":"Fabian M Troschel, Benjamin O Troschel, Maren Kloss, Johanna Jost, Niklas B Pepper, Amelie S Völk-Troschel, Rainer G Wiewrodt, Walter Stummer, Dorothee Wiewrodt, Hans Theodor Eich","doi":"10.1007/s00066-024-02225-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Sarcopenia may complicate treatment in cancer patients. Herein, we assessed whether sarcopenia measurements derived from radiation planning computed tomography (CT) were associated with complications and tumor progression during radiochemotherapy for glioblastoma.</p><p><strong>Methods: </strong>Consecutive patients undergoing radiotherapy planning for glioblastoma between 2010 and 2021 were analyzed. Retrocervical muscle cross-sectional area (CSA) was measured via threshold-based semi-automated radiation planning CT analysis. Patients in the lowest sex-specific quartile of muscle measurements were defined as sarcopenic. We abstracted treatment characteristics and tumor progression from the medical records and performed uni- and multivariable time-to-event analyses.</p><p><strong>Results: </strong>We included 363 patients in our cohort (41.6% female, median age 63 years, median time to progression 7.7 months). Sarcopenic patients were less likely to receive chemotherapy (p < 0.001) and more likely to be treated with hypofractionated radiotherapy (p = 0.005). Despite abbreviated treatment, they more often discontinued radiotherapy (p = 0.023) and were more frequently prescribed corticosteroids (p = 0.014). After treatment, they were more often transferred to inpatient palliative care treatment (p = 0.035). Finally, progression-free survival was substantially shorter in sarcopenic patients in univariable (median 5.1 vs. 8.4 months, p < 0.001) and multivariable modeling (hazard ratio 0.61 [confidence interval 0.46-0.81], p = 0.001).</p><p><strong>Conclusion: </strong>Sarcopenia is a strong risk factor for treatment discontinuation and reduced progression-free survival in glioblastoma patients. We propose that sarcopenic patients should receive intensified supportive care during radiotherapy and during follow-up as well as expedited access to palliative care.</p>","PeriodicalId":21998,"journal":{"name":"Strahlentherapie und Onkologie","volume":" ","pages":"774-784"},"PeriodicalIF":2.5000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11343971/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Strahlentherapie und Onkologie","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00066-024-02225-7","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/28 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Sarcopenia may complicate treatment in cancer patients. Herein, we assessed whether sarcopenia measurements derived from radiation planning computed tomography (CT) were associated with complications and tumor progression during radiochemotherapy for glioblastoma.
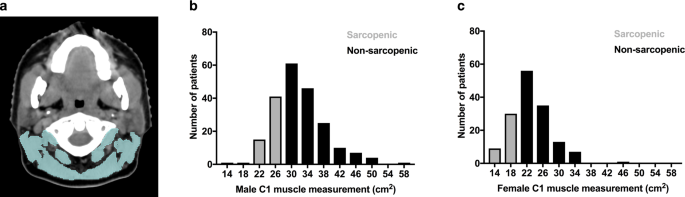
Methods: Consecutive patients undergoing radiotherapy planning for glioblastoma between 2010 and 2021 were analyzed. Retrocervical muscle cross-sectional area (CSA) was measured via threshold-based semi-automated radiation planning CT analysis. Patients in the lowest sex-specific quartile of muscle measurements were defined as sarcopenic. We abstracted treatment characteristics and tumor progression from the medical records and performed uni- and multivariable time-to-event analyses.
Results: We included 363 patients in our cohort (41.6% female, median age 63 years, median time to progression 7.7 months). Sarcopenic patients were less likely to receive chemotherapy (p < 0.001) and more likely to be treated with hypofractionated radiotherapy (p = 0.005). Despite abbreviated treatment, they more often discontinued radiotherapy (p = 0.023) and were more frequently prescribed corticosteroids (p = 0.014). After treatment, they were more often transferred to inpatient palliative care treatment (p = 0.035). Finally, progression-free survival was substantially shorter in sarcopenic patients in univariable (median 5.1 vs. 8.4 months, p < 0.001) and multivariable modeling (hazard ratio 0.61 [confidence interval 0.46-0.81], p = 0.001).
Conclusion: Sarcopenia is a strong risk factor for treatment discontinuation and reduced progression-free survival in glioblastoma patients. We propose that sarcopenic patients should receive intensified supportive care during radiotherapy and during follow-up as well as expedited access to palliative care.
期刊介绍:
Strahlentherapie und Onkologie, published monthly, is a scientific journal that covers all aspects of oncology with focus on radiooncology, radiation biology and radiation physics. The articles are not only of interest to radiooncologists but to all physicians interested in oncology, to radiation biologists and radiation physicists. The journal publishes original articles, review articles and case studies that are peer-reviewed. It includes scientific short communications as well as a literature review with annotated articles that inform the reader on new developments in the various disciplines concerned and hence allow for a sound overview on the latest results in radiooncology research.
Founded in 1912, Strahlentherapie und Onkologie is the oldest oncological journal in the world. Today, contributions are published in English and German. All articles have English summaries and legends. The journal is the official publication of several scientific radiooncological societies and publishes the relevant communications of these societies.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
