Wen Zheng, Xin Huang, Xiao Wang, Min Suo, Yan Yan, Wei Gong, Hui Ai, Bin Que, Shaoping Nie
{"title":"Impact of multimorbidity patterns on outcomes and treatment in patients with coronary artery disease.","authors":"Wen Zheng, Xin Huang, Xiao Wang, Min Suo, Yan Yan, Wei Gong, Hui Ai, Bin Que, Shaoping Nie","doi":"10.1093/ehjopen/oeae009","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>With an aging population and better survival rates, coronary artery disease (CAD) with multimorbidity has become more prevalent, complicating treatment and impacting life quality and longevity. This study identifies multimorbidity patterns in CAD patients and their effect on clinical outcomes, emphasizing treatment strategies.</p><p><strong>Methods and results: </strong>The study analysed data from the DCEM registry (173 459 patients) and BleeMACS cohort (15 401 patients) to categorize CAD patients into three multimorbidity patterns. The focus was on how these patterns influence outcomes, especially concerning the efficacy and safety of dual antiplatelet therapy (DAPT). The study identified three distinct multimorbidity patterns: Class 1 encompassed cardiovascular-kidney-metabolic comorbidities indicating the highest risk; Class 2 included hypertension-dyslipidaemia comorbidities, reflecting intermediate risk; and Class 3 involved non-specific comorbidities, indicating the lowest risk. Class 1 patients demonstrated a six-fold increase in in-hospital mortality and a four-fold increase in severe in-hospital complications compared with Class 3. Over a 1-year period, Class 1 was associated with the highest risk, displaying a significant increase in all-cause mortality [adjusted hazard ratio (HR) 1.87, 95% confidence interval (CI) 1.52-2.31, <i>P</i> < 0.001] and a notable risk for major bleeding (adjusted HR 1.74, 95% CI 1.36-2.24, <i>P</i> < 0.001) compared with Class 3. The use of DAPT, particularly aspirin combined with clopidogrel, significantly reduced the 1-year all-cause mortality in Class 1 patients (adjusted HR 0.60, 95% CI 0.37-0.98, <i>P</i> = 0.04) without increasing in major bleeding.</p><p><strong>Conclusion: </strong>Coronary artery disease patients with a cardiovascular-kidney-metabolic profile face the highest mortality risk. Targeted DAPT, especially aspirin and clopidogrel, effectively lowers mortality without significantly raising bleeding risks.</p><p><strong>Registration: </strong>DCEM registry (NCT05797402) and BleeMACS registry (NCT02466854).</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"4 2","pages":"oeae009"},"PeriodicalIF":0.0000,"publicationDate":"2024-03-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10970685/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeae009","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: With an aging population and better survival rates, coronary artery disease (CAD) with multimorbidity has become more prevalent, complicating treatment and impacting life quality and longevity. This study identifies multimorbidity patterns in CAD patients and their effect on clinical outcomes, emphasizing treatment strategies.
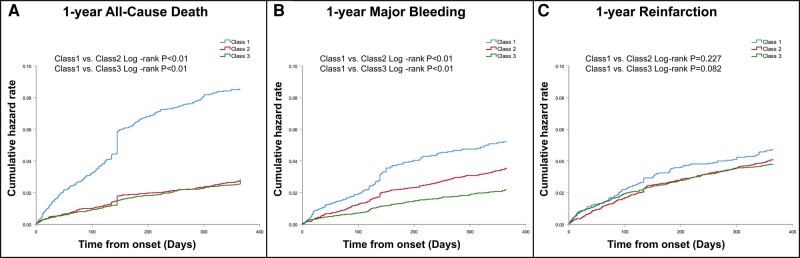
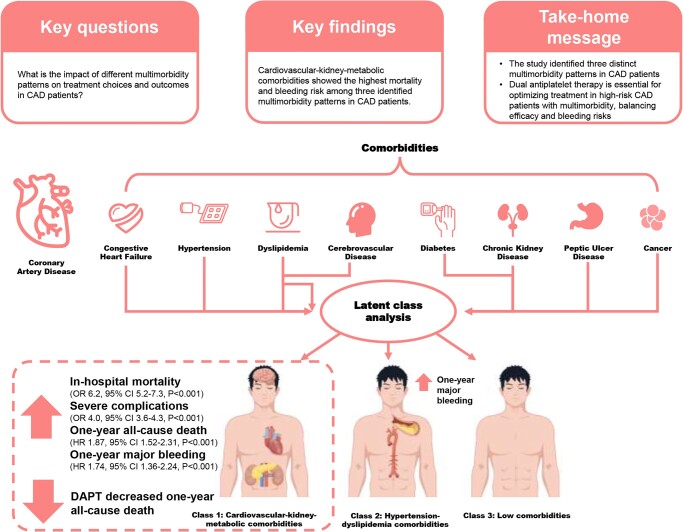
Methods and results: The study analysed data from the DCEM registry (173 459 patients) and BleeMACS cohort (15 401 patients) to categorize CAD patients into three multimorbidity patterns. The focus was on how these patterns influence outcomes, especially concerning the efficacy and safety of dual antiplatelet therapy (DAPT). The study identified three distinct multimorbidity patterns: Class 1 encompassed cardiovascular-kidney-metabolic comorbidities indicating the highest risk; Class 2 included hypertension-dyslipidaemia comorbidities, reflecting intermediate risk; and Class 3 involved non-specific comorbidities, indicating the lowest risk. Class 1 patients demonstrated a six-fold increase in in-hospital mortality and a four-fold increase in severe in-hospital complications compared with Class 3. Over a 1-year period, Class 1 was associated with the highest risk, displaying a significant increase in all-cause mortality [adjusted hazard ratio (HR) 1.87, 95% confidence interval (CI) 1.52-2.31, P < 0.001] and a notable risk for major bleeding (adjusted HR 1.74, 95% CI 1.36-2.24, P < 0.001) compared with Class 3. The use of DAPT, particularly aspirin combined with clopidogrel, significantly reduced the 1-year all-cause mortality in Class 1 patients (adjusted HR 0.60, 95% CI 0.37-0.98, P = 0.04) without increasing in major bleeding.
Conclusion: Coronary artery disease patients with a cardiovascular-kidney-metabolic profile face the highest mortality risk. Targeted DAPT, especially aspirin and clopidogrel, effectively lowers mortality without significantly raising bleeding risks.
Registration: DCEM registry (NCT05797402) and BleeMACS registry (NCT02466854).


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
