{"title":"When and how to use ambulatory blood pressure monitoring and home blood pressure monitoring for managing hypertension.","authors":"Eun Mi Lee","doi":"10.1186/s40885-024-00265-w","DOIUrl":null,"url":null,"abstract":"<p><p>Many individuals have different blood pressure (BP) values in the office setting compared to that outside the office setting. Therefore, confirming hypertension based on office BP (OBP) measurement alone can lead to misdiagnosis and mistreatment. The limitations of OBP measurement have led to the complementary use of out-of-office BP measurements, including 24-hour ambulatory blood pressure monitoring (ABPM) and home blood pressure monitoring (HBPM). This review aims to describe when and how ABPM or HBPM can be used to accurately diagnose and treat hypertension. Both methods should be performed using validated automated oscillometric devices. To minimize user errors, ABPM should be performed using standard techniques, whereas HBPM requires patient education regarding proper BP measurements. ABPM provides short-term comprehensive information on BP, including daytime, nighttime, morning, and 24-h BP. Therefore, ABPM is recommended for the initial diagnosis of hypertension, assessment of BP phenotypes and circadian patterns, and detection of nocturnal hypertension, Furthermore, ABPM plays a critical role in confirming true resistant hypertension thereby excluding pseudo-resistant hypertension. However, it is not suitable for long-term follow-up of patients with hypertension. In contrast, HBPM involves multiple BP readings taken at specific times during the day and evening over a long period. Therefore, HBPM is recommended for diagnosing hypertension and assessing BP phenotypes. However, this method has limitations in measuring nocturnal BP and circadian BP patterns. HBPM is preferred over ABPM for the long-term follow-up of patients with hypertension. This approach improves patient adherence to treatment and ultimately enhances the rate of control of hypertension. Additionally, both methods play an important role in diagnosing and treating white coat hypertension during pregnancy. Consequently, out-of-office BP measurement is essential to prevent the misdiagnosis and mistreatment of hypertension. However, these two methods offer different information regarding the BP status of an individual, and they indeed show discrepancies in the diagnosis of hypertensive phenotypes. Therefore, it is crucial to understand the advantages and limitations of both ABPM and HBPM to ensure their appropriate use in clinical practice.</p>","PeriodicalId":10480,"journal":{"name":"Clinical Hypertension","volume":"30 1","pages":"10"},"PeriodicalIF":3.6000,"publicationDate":"2024-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10983625/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Hypertension","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40885-024-00265-w","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 0
Abstract
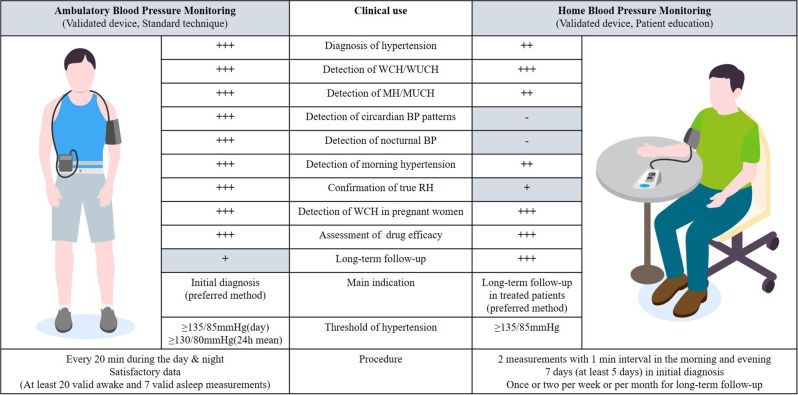
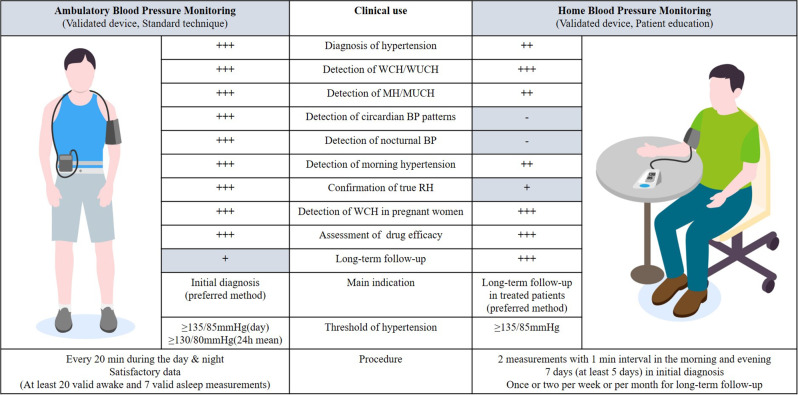
Many individuals have different blood pressure (BP) values in the office setting compared to that outside the office setting. Therefore, confirming hypertension based on office BP (OBP) measurement alone can lead to misdiagnosis and mistreatment. The limitations of OBP measurement have led to the complementary use of out-of-office BP measurements, including 24-hour ambulatory blood pressure monitoring (ABPM) and home blood pressure monitoring (HBPM). This review aims to describe when and how ABPM or HBPM can be used to accurately diagnose and treat hypertension. Both methods should be performed using validated automated oscillometric devices. To minimize user errors, ABPM should be performed using standard techniques, whereas HBPM requires patient education regarding proper BP measurements. ABPM provides short-term comprehensive information on BP, including daytime, nighttime, morning, and 24-h BP. Therefore, ABPM is recommended for the initial diagnosis of hypertension, assessment of BP phenotypes and circadian patterns, and detection of nocturnal hypertension, Furthermore, ABPM plays a critical role in confirming true resistant hypertension thereby excluding pseudo-resistant hypertension. However, it is not suitable for long-term follow-up of patients with hypertension. In contrast, HBPM involves multiple BP readings taken at specific times during the day and evening over a long period. Therefore, HBPM is recommended for diagnosing hypertension and assessing BP phenotypes. However, this method has limitations in measuring nocturnal BP and circadian BP patterns. HBPM is preferred over ABPM for the long-term follow-up of patients with hypertension. This approach improves patient adherence to treatment and ultimately enhances the rate of control of hypertension. Additionally, both methods play an important role in diagnosing and treating white coat hypertension during pregnancy. Consequently, out-of-office BP measurement is essential to prevent the misdiagnosis and mistreatment of hypertension. However, these two methods offer different information regarding the BP status of an individual, and they indeed show discrepancies in the diagnosis of hypertensive phenotypes. Therefore, it is crucial to understand the advantages and limitations of both ABPM and HBPM to ensure their appropriate use in clinical practice.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
