{"title":"Impact of nutritional support routes on mortality in acute pancreatitis: A network meta-analysis of randomized controlled trials","authors":"Ping-Han Hsieh, Tsung-Chieh Yang, Enoch Yi-No Kang, Pei-Chang Lee, Jiing-Chyuan Luo, Yi-Hsiang Huang, Ming-Chih Hou, Shih-Ping Huang","doi":"10.1111/joim.13782","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Nutritional administration in acute pancreatitis (AP) management has sparked widespread discussion, yet contradictory mortality results across meta-analyses necessitate clarification. The optimal nutritional route in AP remains uncertain. Therefore, this study aimed to compare mortality among nutritional administration routes in patients with AP using consistency model.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This study searched four major databases for relevant randomized controlled trials (RCTs). Two authors independently extracted and checked data and quality. Network meta-analysis was conducted for estimating risk ratios (RRs) with 95% confidence interval (CI) based on random-effects model. Subgroup analyses accounted for AP severity and nutrition support initiation.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>A meticulous search yielded 1185 references, with 30 records meeting inclusion criteria from 27 RCTs (<i>n</i> = 1594). Pooled analyses showed the mortality risk reduction associated with nasogastric (NG) (RR = 0.34; 95%CI: 0.16–0.73) and nasojejunal (NJ) feeding (RR = 0.46; 95%CI: 0.25–0.84) in comparison to nil per os. Similarly, NG (RR = 0.45; 95%CI: 0.24–0.83) and NJ (RR = 0.60; 95%CI: 0.40–0.90) feeding also showed lower mortality risk than total parenteral nutrition. Subgroup analyses, stratified by severity, supported these findings. Notably, the timing of nutritional support initiation emerged as a significant factor, with NJ feeding demonstrating notable mortality reduction within 24 and 48 h, particularly in severe cases.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>For severe AP, both NG and NJ feeding appear optimal, with variations in initiation timings. NG feeding does not appear to merit recommendation within the initial 24 h, whereas NJ feeding is advisable within the corresponding timeframe following admission. These findings offer valuable insights for optimizing nutritional interventions in AP.</p>\n </section>\n </div>","PeriodicalId":196,"journal":{"name":"Journal of Internal Medicine","volume":"295 6","pages":"759-773"},"PeriodicalIF":9.2000,"publicationDate":"2024-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Internal Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/joim.13782","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Nutritional administration in acute pancreatitis (AP) management has sparked widespread discussion, yet contradictory mortality results across meta-analyses necessitate clarification. The optimal nutritional route in AP remains uncertain. Therefore, this study aimed to compare mortality among nutritional administration routes in patients with AP using consistency model.
Methods
This study searched four major databases for relevant randomized controlled trials (RCTs). Two authors independently extracted and checked data and quality. Network meta-analysis was conducted for estimating risk ratios (RRs) with 95% confidence interval (CI) based on random-effects model. Subgroup analyses accounted for AP severity and nutrition support initiation.
Results
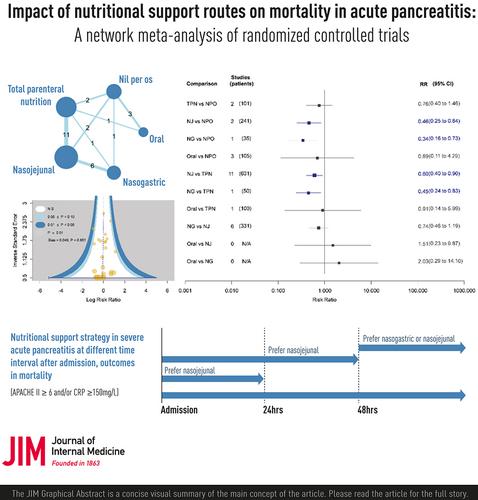
A meticulous search yielded 1185 references, with 30 records meeting inclusion criteria from 27 RCTs (n = 1594). Pooled analyses showed the mortality risk reduction associated with nasogastric (NG) (RR = 0.34; 95%CI: 0.16–0.73) and nasojejunal (NJ) feeding (RR = 0.46; 95%CI: 0.25–0.84) in comparison to nil per os. Similarly, NG (RR = 0.45; 95%CI: 0.24–0.83) and NJ (RR = 0.60; 95%CI: 0.40–0.90) feeding also showed lower mortality risk than total parenteral nutrition. Subgroup analyses, stratified by severity, supported these findings. Notably, the timing of nutritional support initiation emerged as a significant factor, with NJ feeding demonstrating notable mortality reduction within 24 and 48 h, particularly in severe cases.
Conclusion
For severe AP, both NG and NJ feeding appear optimal, with variations in initiation timings. NG feeding does not appear to merit recommendation within the initial 24 h, whereas NJ feeding is advisable within the corresponding timeframe following admission. These findings offer valuable insights for optimizing nutritional interventions in AP.
期刊介绍:
JIM – The Journal of Internal Medicine, in continuous publication since 1863, is an international, peer-reviewed scientific journal. It publishes original work in clinical science, spanning from bench to bedside, encompassing a wide range of internal medicine and its subspecialties. JIM showcases original articles, reviews, brief reports, and research letters in the field of internal medicine.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
